 Health insurance coverage is a critical factor in making health care affordable and accessible to women. Among the 97.4 million women ages 19 to 64 residing in the U.S., most had some form of coverage in 2017. However, gaps in private sector and publicly-funded programs left a little over one in ten women uninsured. The Affordable Care Act (ACA) expanded access to coverage through a combination of Medicaid expansions, private insurance reforms, and premium tax credits. This factsheet reviews major sources of coverage for women residing in the U.S. in 2017, discusses the impact of the ACA on women’s coverage, and the coverage challenges that many women continue to face.
Sources of Health Insurance Coverage Employer-Sponsored Insurance
Non-Group Insurance The ACA expanded access to the non-group or individually purchased insurance market by offering premium tax credits to help individuals purchase coverage in state-based health insurance Marketplaces. It also included many insurance reforms to alleviate some of the long-standing barriers to coverage in the non-group insurance market. In 2017, about 9% of non-elderly adult women (approximately 8.4 million women) purchased insurance on their own.3 This includes women who purchased private policies from the ACA Marketplace in their state, as well as from private insurers that operate outside of Marketplaces.
The state-federal program for low-income individuals, Medicaid, covered 17% of non-elderly adult women in 2017. Historically, to qualify for Medicaid, women had to have very low incomes and be in one of Medicaid’s eligibility categories: pregnant, mothers of children 18 and younger, disabled, or be over 65. Women who didn’t fall into these categories typically were not eligible regardless of how poor they were. The ACA allowed states to eliminate these categorical requirements and broaden Medicaid eligibility to most individuals with incomes less than 138% of the FPL regardless of their family or disability status or age, effective January 2014. As of December 2018, 36 states and DC have taken up this option.
Uninsured Women Approximately 11% of women ages 19 to 64 (approximately 10.6 million women) were uninsured in 2017, a decline from a rate of 19% in 2013. Uninsured women often have inadequate access to care, get a lower standard of care when they are in the health system, and have poorer health outcomes. Compared to women with insurance, uninsured women have lower use of important preventive services such as mammograms, Pap tests, and timely blood pressure checks. They are also less likely to report having a regular doctor. Low-income women, women of color, and immigrant women are at greater risk of being uninsured. One in five women with incomes under 200% of the FPL ($24,100 for a single individual) are uninsured, compared to just 7% of women with incomes over 200% FPL. Single mothers are more likely to be uninsured (13%) than women in two-parent households (10%).
Many women who are uninsured are potentially eligible for coverage, but are not enrolled. Some, however, still lack any pathway to affordable coverage. Over half of uninsured women are eligible for either Medicaid or tax subsidies under the ACA. One in five (2.1 million) uninsured women are low-income and currently eligible for Medicaid but are not enrolled and another third (3.5 million) are income eligible for a subsidized Marketplace plan but not enrolled
Scope of Coverage and Affordability The ACA set national standards for the scope of benefits offered in private plans. In addition to the broad categories of essential health benefits (EHBs) offered by marketplace plans, all privately-purchased plans must cover maternity care and mental health, which had been historically excluded from most those plans. In addition, most private plans must cover preventive services without co-payments or other cost sharing. This includes screenings for breast and cervical cancers, well woman visits (including prenatal visits), prescribed contraceptives, breastfeeding supplies and supports such as breast pumps, and several STI services. However, the Trump administration’s expansion of short-term plans that do not have to comply with any of these benefits standards could erode the scope of coverage some women receive. Additionally, on November 15, 2018, the Trump Administration issued final regulations expanding the type of employers that may be exempt from the ACA’s contraceptive coverage requirements to include any private employer with a religious or moral objection to contraception. Women who work for exempt employers and female dependents will no longer be entitled to contraceptive coverage. Abortion services are explicitly prohibited from being included as EHBs. Twenty-six states have laws banning coverage of most abortions from the plans available through the state Marketplaces, and plans offered in states that don’t ban coverage must segregate payments for abortion coverage. Affordability of coverage and care continues to be a significant concern for many women, both for those who are uninsured as well as those with coverage. The leading reason why uninsured women report that they haven’t obtained coverage is that it is too expensive. Under employer-sponsored insurance, the major source of coverage for women, 58% of all covered workers have deductibles of at least $1,000. Similar affordability challenges exist in the non-group market, which includes the ACA Marketplaces. Forty-seven percent report dissatisfaction with their plan’s annual deductible, and 43% are dissatisfied with their monthly premium. Looking Forward Health coverage matters for women. Those with health coverage are more likely to obtain needed preventive, primary, and specialty care services, and have better access to new advances in women’s health. Today, women can get coverage without worrying that they will be charged more for insurance than men, be assured that their insurance provides them with no-cost coverage for a wide range of recommended preventive services, and coverage for critical services for women such as maternity care and mental health. While there has been much progress in expanding coverage and reducing the number of uninsured women since the passage of the ACA, affordability continues to be a challenge for many women and 10.6 million women still lack coverage. About half of uninsured women qualify for either Medicaid or subsidies to secure coverage through the health care exchanges but many still lack a pathway to affordable coverage. Recent state and federal efforts to roll back ACA-related policies will likely erode the gains in coverage experienced by millions of women in recent years. In particular, the repeal of the individual insurance mandate, reduced resources for outreach and enrollment for individuals to enroll in Marketplace coverage, and policies that destabilize the individual insurance market will undermine many coverage improvements. In addition, efforts to expand the availability of insurance products like short-term plans that do not offer the full range of essential health benefits such as maternity care and preventive services will serve to weaken coverage and could result in higher out-of-pocket costs for women who need these services. Women will continue to have much at stake in the outcomes of the ongoing health care debates in Washington DC and in state capitols across the nation. Your chip application pa is based on your household size and income and determined by the government and you can apply any time of year.
2 Comments
 After his son was hit by a car in San Francisco and taken away by ambulance, Karl Sporer was surprised to get a bill for $800.
Mr. Sporer had health insurance, which paid for part of the ride. But the ambulance provider felt that amount wasn’t enough, and billed the Sporer family for the balance. “I paid it quickly,” Mr. Sporer said. “They go to collections if you don’t.” That was 15 years ago, but ambulance companies around the nation are still sending such surprise bills to customers, as Mr. Sporer knows well. These days, he oversees the emergency medical services in neighboring Alameda County. The contract his county negotiated allows a private ambulance company to send similar bills to insured patients. In most parts of medical care, you can choose a doctor or hospital that takes your insurance. But there are some types of care where politicians have begun tackling the “surprise” bills that occur when, say, patients go to an emergency room covered by their insurance and are treated by a physician who is not. Five states have passed laws this year to restrict surprise billing in hospitals and doctor’s offices. Congress is working on a similar package of measures, after President Trump held a news conference in May urging action on the issue. But none of these new policies will protect patients from surprise bills like the one Mr. Sporer received. Ordinary ambulances that travel on roads have been left out of every bill. “Ambulances seem to be the worst example of surprise billing, given how often it occurs,” said Christopher Garmon, a health economist at the University of Missouri-Kansas City. “If you call 911 for an ambulance, it’s basically a coin flip whether or not that ambulance will be in or out of network.” Ambulances: The Largest Source of Unexpected Medical Bills Mr. Garmon’s research finds that 51 percent of ground ambulance rides will result in an out-of-network bill. For emergency room visits, that figure stands at only 19 percent. Congress has shown little appetite to include ambulances in a federal law restricting surprise billing. One proposal would bar surprise bills from air ambulances, helicopters that transport patients who are at remote sites or who have life-threatening injuries. (These types of ambulances tend to be run by private companies.) But that interest has not extended to more traditional ambulance services — in part because many are run by local and municipal governments. Lamar Alexander, the chairman of the Senate Committee on Health, Education, Labor and Pensions, and a key author of a Senate surprise billing proposal, said in an email that surprise bills from air ambulances were the more pressing issue because federal law prevents any local regulation of their prices. “Unlike air ambulances, ground ambulances can be regulated by states,” said Mr. Alexander, a Republican from Tennessee. “And Congress should continue to learn more about how to best solve that problem.” The ambulance industry has brought its case to Capitol Hill, arranging meetings between members of Congress and their local ambulance operators. “When we talk to our members of Congress, what we really emphasize is that we’re a little different from the other providers in the surprise billing discussion,” said Shawn Baird, president-elect of the American Ambulance Association. “We have a distinct, public process. The emergency room isn’t subject to any oversight of that kind.” Patient advocates contend that this public oversight isn’t doing enough to protect patients, who often face surprise bills and forceful collection tactics from ambulance providers. Anthony Wright, executive director of Health Access California, worked on a 2016 California law to restrict surprise billing. Initially, he thought it made sense to include ambulances in that legislation. “It’s our experience that ambulance providers bill quicker and are more aggressive in sending bills to collection,” Mr. Wright said. “If they’re being more aggressive, you might want legislation to deal with that one first.” But obstacles quickly began to mount. Some were about policy, like whether California would need to offset the revenue local governments would lose. Then there were the politics. “There is the political reality that it’s hard to go after an entire industry at once,” Mr. Wright said. “It’s hard to have a bill opposed by doctors and hospitals and ambulances. We did manage to get a strong protection against doctor billing, but that was an epic, brutal, three-year fight.” The California law that passed in 2016 did not regulate ambulance prices. Patient groups elsewhere also say they ran into political trouble. Of the five states that passed surprise billing regulations in 2019, only Colorado’s new law takes aim at ambulance billing — not by regulating it, but by forming a committee to study the issue. “The surprise bills laws are hard enough to get,” said Chuck Bell, program director for advocacy at Consumer Reports, who worked to pass a Florida surprise billing law in 2016. “You’re struggling with health plans, hospitals and doctors and other provider groups. At a certain point you don’t want to invite another big gorilla in the room to further widen the brawl.” On Capitol Hill, the ambulance services have been less aggressive than other health care providers in lobbying against their inclusion in reforms. But lawmakers have largely declined to even include them in the conversation. Consumer advocates say the lack of state-level legislation has been a barrier. “Since there are issues related to ambulances being run by municipalities, and, at the state level, there hasn’t been a lot of model law to inform federal law, I think that’s made some members hesitant to wade into that space,” said Claire McAndrew, the director of campaigns and partnerships at the health care consumer group Families USA. Local governments generally finance their ambulance services through a mix of user fees and taxes. If ambulances charge less to patients, they typically need more government funding. Municipal governments often publish the prices of their ambulance services online, and they can range substantially. In Moraga and Orinda, in the Bay Area, the base rate for an ambulance ride is $2,600, plus $42 for each mile traveled. In Marion County, Fla., the most basic kind of ambulance ride costs $550, plus $11.25 per mile. In many communities, there is no choice of ambulances. Older patients are not charged such fees. Medicare, which also covers some people with disabilities, pays set prices for ambulance rides — a base rate of around $225 for the most typical type of care, in addition to a mileage fee — and forbids the companies to send patients additional bills. In Bucks County, Pa., where it is $1,500 for a basic ambulance ride, in addition to $16 per mile, the emergency medical service gets 78 percent of its revenue from ambulance billing, according to Chuck Pressler, the executive director of the Central Bucks Emergency Medical Services. The rest of the budget comes from taxes raised by local cities and fund-raising drives. “There is an expectation that we just plant money trees, that people should come in and work for free,” Mr. Pressler said of proposals to tamp down ambulance billing. “When was the last time you saw the police send out a fund-raiser? They don’t have to do that. Why do we have to raise money to come get you when you’re sick?” You can easily get best plans by exploring best health insurance harrisburg for you and your family.  A nurse walked in with a loaded syringe. “Can you lift your gown?” she asked.
The woman on the gurney held the scratchy emergency room blanket closer to her chin. “What’s in the syringe?” she asked. The nurse frowned. “Don’t you want the medicine your doctor ordered?” The woman took a deep breath and kept asking questions. She had more than just self-interest on the line. She was a “secret shopper,” a consultant pretending to be a patient in order to evaluate the quality and culture of care in a hospital. Some hospitals — including the one where I work — have hired secret shoppers to pose as patients seeking care, using pseudonyms and symptoms of an illness that cannot be diagnosed or ruled out right away. They describe a psychiatric condition, perhaps, or an intermittent heart arrhythmia. Just like any other patient, the secret shopper wears an open-backed hospital gown and a plastic identification bracelet. A nurse inserts an IV and connects telemetry leads. Next comes the usual parade of phlebotomists, doctors, X-ray techs, orderlies and more. The secret shopper evaluates how compassionately she and other patients are treated. Do nurses wash their hands? Do doctors listen? A trained sociologist who works with a consulting company called Etch Strategies, the secret shopper complements her observations with dozens of systematic interviews with patients, executives, nurses, doctors and beyond. When her analyses are done, she presents her findings to hospital leadership. A few years ago, Randy Peterson, then the president and chief executive of Stormont Vail Health, a medical center in Topeka, Kan., hired Etch Strategies. Mr. Peterson, who retired this spring, said he wanted to figure out why his 586-bed hospital had only average patient satisfaction scores despite getting high marks on clinical quality metrics. The secret shopper found clues. She observed that caregivers were sometimes brusque and even dismissive of patients. They didn’t always interact well with each other, either. More than once, the secret shopper overheard emergency room workers bad-mouthing employees from other areas of the hospital. When N.Y.C. Is Your Gym: Meet the Athletes Redefining Fitness in the City’s Parks I Wanted to Know What White Men Thought About Their Privilege. So I Asked. “They didn’t feel like a team,” she said, “and that made me doubt the quality of my care.” Mr. Peterson said the secret shopper’s presentation of these and other analyses had his leadership team “spellbound.” A plan to make Stormont Vail Health a better place to heal quickly followed. For example, the medical center created new tenets of employee behavior designed to improve the patient experience. Staff members were encouraged to greet people in the hallways rather than thumbing their phones while walking. “Keep your eyes up. Socialize with patients instead of talking about patients. Tune into the social determinants of health. Everyone has a story,” Mr. Peterson said. Secret shoppers have illuminated many aspects of the patient experience. In a 2016 study, secret shoppers contacted 743 primary care practices across California. Over 70 percent were unable to make an appointment with the original clinician they contacted, illustrating how challenging it can be to access health care. Secret shoppers have cut telephone wait times for patients of orthopedics clinics, and this spring a secret shopper study showed that more than a third of patients seeking treatment for opioid addiction were denied an appointment. The experiences of vulnerable patients like these can be highlighted by secret shoppers. A second secret shopper from Etch Strategies presented to an emergency room in rural New York wearing sweatpants and a T-shirt with the name of an indie band. She had not showered for three days and told the desk clerk she didn’t have health insurance. This secret shopper, who in real life works in marketing and qualitative research, said it made her nervous to pretend to be someone else. But the disguise helped her make an important discovery. “From the second I walked in, people were very short with me,” she said. “There was no eye contact. People didn’t even introduce themselves!” At one point, a phlebotomist got the secret shopper’s blood “all over my arm and a sheet.” There was no apology. No explanation. The secret shopper said there was a stark difference between this treatment and the care she has received when fully insured and professionally attired. Secret shoppers do expose themselves to some risk, such as blood draws, an IV, maybe even an X-ray. They decline more invasive tests and interventions, though, pleading a scheduling conflict or urgent family matter if the risks become too great. Hospital leaders pore over reams of data. They review financial spreadsheets, patient satisfaction surveys and clinical outcome data. Secret shopper studies don’t replace that information. Rather, they attempt to give the data context. “Stories move data from the head to the heart,” said Kristin Baird, president and chief executive of the Baird Group, a Wisconsin-based company that performs secret shopper and other consulting services for health care organizations. She has seen how patient stories that exemplify otherwise confusing trends in the data can influence health care executives powerfully. Dr. Steve Leffler, an emergency room physician and interim president of the University of Vermont Medical Center, where I work, says he has seen secret shoppers and other work of Etch Strategies enable difficult institutional culture change by showing how clinical care feels to patients and employees. Dr. Leffler says secret shoppers are “a mirror for all of us.” They help bring patient needs to the forefront, and they help clinicians reorient to the fundamental importance of making a human connection with every patient they see. Explore health insurance plans harrisburg and get the best plans for your family, if you want to know more details then please send your queries in the comment section.  As Hurricane Barry made landfall Saturday in Louisiana and later weakened to a tropical storm, the window of opportunity for reducing property risks had already begun closing for residents who don’t have a comprehensive disaster preparedness plan in place.
In fact, a survey in June by the Private Risk Management Association (PRMA) of nearly 100 insurance agents revealed that homeowners continue to be overly optimistic about their safety and property in the event of a natural disaster. Seventy percent of agents stated that fewer than 50% of their clients evacuate when a category 3 hurricane or greater is forecast to significantly affect their region. Sixty-five percent say less than 10% of their clients take proactive measures, or risk mitigation plans, to protect their property such as installing inflatable barriers to prevent flood waters from entering the homes or moving collectibles and other valuables to a secure off-site location. Eighty-six percent of the survey respondents believe that fewer than 50% of their clients have a comprehensive hurricane preparedness plan, and 50% state that their clients only update their disaster plans after being affected by a weather event. “With this tropical storm brewing, the availability to get or change insurance will dramatically change,” said Lisa Lindsay, executive director of PRMA, a nonprofit educational organization that aims to educate insurance agents so they can better advise homeowners. “What will happen is insurance companies will stop binding coverages,” she said, explaining that homeowners would be prevented from getting new coverage put in place. “You won’t be able to go out and get a flood policy because there is a 30-day waiting period,” said Lindsay. “Whenever there is a pending storm or hurricane, it dramatically changes the ability to change or get new insurance, which is why we recommend disaster preparedness planning.” In 2018, there were 11 weather disaster events in the United States that had losses exceeding $1 billion, according to the National Oceanic and Atmospheric Administration. “Homeowners tend to adopt the mindset that it’s not going to happen to me because, one, it’s never happened, or I just don’t want to think about it,” said Lindsay. “We’re not seeing people proactively putting together comprehensive preparedness plans. In fact, our survey suggests that a majority of our agents believe that less than 50% of their clients have a comprehensive preparedness plan.” PRMA aims to change that mindset and complacency through education and working with its members. The organization’s survey focused on hurricanes, but Lindsay said the research is applicable to any natural disaster, whether it is the recent earthquakes and aftershocks that have rocked California or twisters in Tornado Alley. “We’ve heard on the news that since California hasn’t been hit with earthquakes in recent years that people have become complacent,” said Lindsay. “They didn’t have their go bags. They didn’t have the necessary things they should have in their home or office should an earthquake hit. So we believe that through education and talking about these things that we can help people be better prepared for whatever emergency lies ahead.” Lindsay says the effects of natural disasters are less severe for residents whose evacuation plans take into consideration what they are going to take with them and how to safeguard as many items as possible that they will leave behind. “People have to take action,” she said. “They shouldn’t just be sitting there waiting for things to progress.” A family might not be together if a disaster strikes, so it is important to know which types of disasters could affect your area and plan accordingly. “If you’re in a hurricane area, you might identify a hurricane, wind storm and flooding as likely to happen,” said Lindsay. “Then you’re going to work on creating an action plan, and that action plan entails who’s going to be responsible for what, whether it’s being in charge of pets, family medications, family contacts, your disaster kit, and then coming up with a detailed communication plan. And by that, we mean ensuring that all family members are accounted for or safely have access to necessary resources. All of those plans take into account personal safety and protection of property.” Ready.gov, the official website of the Department of Homeland Security, offers a guide for creating an emergency plan before a disaster strikes. A new breed of mobile disaster apps complements and improves the way federal and local agencies prepare for and deal with emergencies. Lindsay said all homeowners should have some type of flood insurance policy in place, pointing out the recent flash flood emergency in Washington, D.C. as an example of a weather-related threat that could happen anywhere. “All 50 states have experienced flood disasters, and everyone lives in a flood zone regardless of whether they live near a body of water,” she explained. “If you think about the way people think of flooding historically through the National Flood Insurance Program, there are high-risk areas, and there are lower-risk areas,” said Lindsay. “So every area ends up being mapped out in a flood zone. Our theory is that FEMA (Federal Emergency Management Agency) and the way they have mapped out flood zones is antiquated because they are not taking into account a lot of the other parameters like the effect of storm surge. They are not taking into account the parameters on the changes in soil density and runoffs. There are firms that can do a more comprehensive flood risk mapping, and that’s a more realistic indication of their flood risk than relying on the National Flood Insurance Program.” Documenting insurance claims is a good reason for maintaining an inventory of your household goods. Lindsay recommends using smartphone apps to catalog valuable items or creating a video of all of the contents in your home to help verify loss for insurance and taxes. “I liken this whole preparedness discussion to an estate planning discussion,” she said. “We all know we should have an up-to-date estate plan. We all know we should have a will and health care directives and all that. But the last time I spoke to an estate attorney, she told me that on average 64% of people don’t have an up-to-date estate plan or will. And it’s because it’s not something they are comfortable doing. And I believe that’s the reason some people just don’t jump on putting together a preparedness plan. That’s why we as an association with our members want to lead the charge and help them step by step put this together. Because it’s the same scenario.” If you want to know more about the private health insurance pa then please send your queries by dropping a comment below.  Choosing the right insurance plan — and getting the best rate — can feel daunting. But just because you're content with your current insurance rate doesn’t mean you can’t do anything to improve it, especially as an entrepreneur for whom every cent counts.
If you’re new to the insurance game, it’s particularly important to do your homework before signing up. A little preparation and proactivity can go a long way toward improving your rates. And for business owners looking to establish a solid business credit score, that's essential — especially if their personal credit has started to bleed into their business's. Don’t Be Fooled: The Sneaky Areas That Might Impact Your Insurance Rate Think you have a handle on your insurance? Be sure these areas aren’t secretly affecting your rates: 1. Your insurance (and credit) score Your insurance score — and by extent, your credit score — can be a major predictor of your insurance rate. But why do your insurance and credit scores impact your auto insurance rates? Insurers utilize your insurance score as a predictor of risk, and a big part of your insurance score is looking at your credit history. According to an article in ReadWrite, “your auto insurance score is less concerned with what’s in your financial accounts and more interested in how you interact with them. Your insurance score looks at metrics like age of financial accounts, payment history, and credit utilization.” The higher your score, the more likely it is that providers will see you as responsible — and that you’ll see lower rates as a result. A study by insurance Quotes found that consumers with a poor credit score paid for it in their premiums, with their rates nearly doubling. That’s why it pays to keep tabs on your credit and auto insurance scores. One place to start is by requesting your credit report annually and reviewing it for errors. Make sure if you’re being penalized, it’s actually for mistakes you made. You can access your insurance score on personal finance sites like Credit Karma, and some providers like Say Insurance will allow anyone to check their insurance score for free. 2. Where you live With a majority of accidents happening close to home, where you live can actually impact your insurance rates. Some cities and neighborhoods that are known to have higher rates of theft, accidents, and uninsured drivers will also often have higher insurance rates. Plus, cities tend to boast more accidents than rural areas, which means your rates will reflect that increase in accidents. It’s also common for areas with higher unemployment rates to have higher insurance rates because it’s more likely that you may be uninsured. Even a lengthy commute can cause an increase in your rates. In contrast, home ownership can sometimes factor positively into your rate assessment. Some companies, like Travelers Insurance, give homeowners a discount on their auto insurance. You might not even have to buy your homeowners insurance through the same company, although it can certainly help your rates if you bundle. 3. What you drive You might not have thought about it when you were shopping for a new car, but the type (and age) of car you drive directly affects how much you pay in insurance. When assessing your risk, providers often assign a higher rate to cars that go faster. That fancy sports car, while it might up your cool factor, will also increase your premium. That doesn’t always mean your older car is saving you money. In fact, if you have an older car and are still carrying collision coverage, you could be losing money. Even though significant repair costs can often be the same, it’s more common for older cars to be considered totaled in an accident because the cost of the repairs can often exceed the value of the car itself. It’s why having collision coverage on your new car is so important; the cost to replace it will be much higher. But if your car is worth less than several thousand dollars, you could actually end up paying more than it’s worth in collision coverage. 4. Your marital status, age, and gender Young men, particularly those in their teens and early twenties, have some of the highest insurance rates (and some of the highest accident rates, creating the correlation). If your teen recently hit the road, it might be in your benefit to make sure that their grades stay up. Some insurance companies offer a rate discount to young drivers that make the honor roll or dean’s list, or who have a high grade point average or standardized testing scores. Similarly, marriage is another factor that can lower insurance rates for customers, particularly if they're in their twenties. Insurance companies have found that married people often have fewer accidents and file fewer claims than single individuals, in part because merging households often means merging vehicles, too. 5. Your work You read that right — your insurance rate might actually be influenced by your work. The logic is as follows: The more your job requires you to drive, the more likely it is that you might be in an accident. It’s also important to take into account the time of day that you're most likely to be behind the wheel. A new study has shown that entertainers are most likely to have a higher insurance rate. This includes actors, musicians, athletes and — with the highest rate — circus workers. On the other end of the spectrum, people who regularly deal with numbers as part of their profession are less likely to pay a costly insurance premium. Entrepreneurs trying to wrap their heads around insurance would do well to consider how the details of their lives — and work — impact their insurance score. Finding ways to pay as little as possible — for damages or upfront rates — can truly help business owners stay financially healthy. Get insured your whole family by exploring the family health plan york and if you want to know more then please contact us in the comment section.  In an ideal world, most people would own their own health insurance and take it with them as they travel from job to job and in and out of the labor market. Some employers may have better insurance than people can find in the open market. But most employers would prefer to make a cash contribution to help employees pay their own premiums rather than provide insurance directly.Before there was Obamacare, this is what some employers were actually doing. They used an account called a Health Reimbursement Arrangement (HRA), providing funds employees could use to buy their own health insurance. These funds were not taxed as income to the employee, just as employer-provided insurance isn’t taxed. There was always legal uncertainty about this practice, however. Many insurance agents were fearful that if they knew the policies they sold were being purchased with employer money, they could be penalized. So, it was common practice for everyone to act on the principle of “don’t ask; don’t tell.” Then came Obamacare. The Obama administration didn’t just dislike the practice of employers helping employees obtain their own insurance. They hated the idea. An Obama regulation stipulated that employers caught giving their employees pre-tax dollars to purchase their own coverage could be fined as much as $100 per day for each employee, or $36,500 a year. This was the highest penalty in all of Obamacare regulations. Thankfully, the Trump administration is eliminating this penalty and much more. Beginning next January, employers will be able to use HRAs to help employees obtain their own coverage with the administration’s blessing. This regulatory change is coming at the right time. Readers may be surprised to learn that the extent of private insurance coverage has gone down under Obamacare, despite huge federal subsidies in the individual market and a government mandate requiring most employers to offer coverage. The biggest losses are among small businesses. Among firms that employ 3-24 workers, the percentage of employees covered by employer health benefits fell from 44% in 2010 to 30% in 2018. Among firms that employ 24-29 workers, the percentage fell from 59% in 2010 to 44% in 2018. Moreover, 27% of employees of small and medium-sized firms (3 to 199 workers) turn down their employer’s offer of health insurance. This is probably because Obamacare mandates have made all insurance more expensive and less attractive. Will employees be able to find better coverage in today’s individual market? That may depend on where they live. An acquaintance of mine in New York City has seen her individual market premium jump fivefold in the past four years. She now pays more than $25,000 for a family coverage with a high deductible and increasingly narrow network of providers. Not many employees will envy her experience. Some states, however, have obtained Obamacare waivers. By using dedicated funds for high-cost enrollees, they are allowing premiums to fall for everyone else. Employees may also benefit because of another Trump administration change. Employers are allowed to deposit up to $1,800 a year in an “excepted benefit HRA” and these funds can be used to purchase short-term, limited-duration insurance. This insurance does not have to comply with Obamacare regulations, including their prohibition on basing premiums on the health condition of the applicant. Traditionally, such plans only lasted up to one year and they were purchased by people who were transitioning between jobs or from school to work. To discourage their use the Obama administration limited these plans to three months’ duration. However, the Trump administration has reversed that regulation and extended the duration to three years. It is also allowing people to buy a second kind of insurance that I call “health status insurance.” This second plan protects people from any extra premium they might be charged in a second three-year period, should their health condition deteriorate during the first three-year period. By stringing together these two types of insurance, people will be able to purchase insurance that meets family needs, rather than the needs of bureaucrats and regulators – indefinitely, into the future. People will be able to purchase, say, a Blue Cross plan similar in benefits and price to what they could obtain before there was Obamacare. Note, however, that state governments can sharply curtail these plans and even regulate them out of existence. Several blue states have already done so. In promoting these reforms President Trump is exercising a very aggressive use of executive authority. He is also providing needed leadership to a party that has lost its way when it comes to health policy. In the last several years, the only Republican plan to reform Obamacare that included personal and portable insurance and health status insurance was a bill sponsored by House Rules Committee chairman Pete Sessions and Sen. Bill Cassidy. (Fair disclosure: I helped write it.) The other proposals, including ones preferred by the Republican leadership, did little more than help Obamacare work better. The reforms discussed here were announced by the president at a Rose Garden ceremony. But they were well known (because regulatory changes invite public comments) before the last election. Can you think of a single Republican candidate in last fall’s election who campaigned on these reforms? I can’t. Nor was there even a single congressional hearing designed to showcase the need for the reforms. Trump has also taken on the special interests. Almost all the major players in health policy – especially the large insurance companies – oppose these changes. But just as he took on the pharmaceutical companies on drug prices and the hospitals on price transparency, the president doesn’t seem to hesitate when Big Insurance objects. Executive action can only go so far, however. Obamacare is still law. To fully realize the Trump vision of health reform, Congress needs to act. That means that Republicans and Democrats must ignore all the special interests and support reforms that work for ordinary citizens. It is important to have a health insurance for any individual and you can check your eligibility for catastrophic health insurance pa and explore best plans for you.  SENATOR BERNIE SANDERS recently announced his Medicare-for-All bill. This is basically the senate version of the congressional bill introduced by Pramila Jayapal. The bill would eliminate the insurance industry and much of the billing bureaucracy that exists today. It would provide health care coverage for everyone and eliminate copays and deductibles. It would expand Medicare coverage to include dental, vision and long-term nursing home care. There are many questions about how this approach to universal care would be funded. No budget has been provided, though estimates vary from an annual increase in cost of $3.2 trillion to an annual savings of $600 billion. Jayapal said it would likely require raising taxes on the wealthy, and Sanders suggested this could be up to 70%. Another option could be taxing investment income at the same rate as stock sales. Under the Medicare-for-All plan, private insurance would be eliminated and physicians who are in private practice would be paid on a fee-for-service basis through a national fee schedule, likely at the current Medicare rate or slightly lower. By eliminating the insurance industry, the plan would also eliminate one million jobs. The new fee schedule would be significantly lower than the current industry fee schedule, which means Medicare-for-All would likely lower physician incomes in a significant way, making a bad situation for physicians even worse. There are three basic objections to Medicare-for-All. The first is that taxes would go up, so it would not receive bipartisan support. The second is that it's a vote loser. When Americans are polled, 70% say that they approve of Medicare-for-All. However, when a follow-up question is asked, in which it is made clear that this means everybody would be required to have it, support drops to 38%. The third and perhaps most important objection is that many experienced doctors would simply leave the profession, and this problem is not solved by retaining the commercial insurance corporations, since this is merely retaining a system that needs to change. Physicians are the single most important service provider in any healthcare system, and we are facing a shortage. The Association of American Medical Colleges projects that this shortage will worsen, even without the negative influence of Medicare-for-All. And doctors face the highest burnout rate among all professions -- as many as 46% of doctors in the U.S. have suffered from burnout at some time in their careers, according to Dr. Dike Drummond in his article from Family Practice Management Journal. In our book, "Healing American Healthcare," we describe our Eichhorn-Hutchinson plan. There are six critical objectives that, if achieved, could improve quality while reducing the cost of healthcare by as much $1 trillion per year: 1. Provide universal health care by requiring all employers to provide health insurance for their employees. Establish and provide a national health care option, which we have named Allcare, which would provide the same minimum benefits of the Medicare program. We estimate that the cost of Allcare would be 30% below the average cost of employer-based health insurance today as established by the annual Kaiser Family Foundation Survey. Existing insurers would be invited to compete, and could develop Medicare Advantage-like plans to expand benefit offerings to people under the age of 65. 2. Control drug costs through the establishment of a national negotiating platform that would be shared with all health care systems to prevent and eliminate price gouging in the pharmaceutical industry and unreasonable hospital markups of drugs they administer to their patients. The goal is to reduce the per capita costs of our medications to match the per capita cost of other industrialized democracies. Nonprofit hospitals and nonprofit hospital systems that earn operating profits would be required to pay income tax at the corporate rate. 3. Reduce the complexity and bureaucracy of billing by having a national standard for the cost of care: a national chargemaster for all services provided for patients at any hospital or clinic or doctor's office anywhere in the US regardless of the provider's tax status as for-profit or nonprofit entities. 4. Eliminate hospital facility fees for outpatient testing and standardize all imaging and lab testing fees. While this would be a loss of revenue for hospitals, at the same time hospitals would gain by not having to provide indigent care, since everyone would be insured, and by shedding much of their bureaucratic overhead. 5. Use the health care data that is available to monitor costs, improve quality, and reduce waste, and recommend that Accountable Care Organizations be provided with this data as they work to control costs and improve patient outcomes. 6. Massively reduce the complexity of the Electronic Health Record, or EHR, and EHR-associated measures of efficiency and quality, which are burdensome, insulting and actually reduce efficiency and quality. The EHR is the number one cause of physician burnout – let's let doctors go back to being doctors. We also believe that employers and individuals should have choice in selecting health insurance. Under our plan, employers could be self-insured, contract with private insurance companies or contract with Allcare. In each case they could have Gold, Silver or Bronze plans to expand physician networks for their employees. This layered plan would allow anyone to be insured at the level of basic Medicare, but by paying extra would gain access to larger pools of doctors. Individuals could also choose between Allcare and private insurance. Our proposed plan reduces bureaucracy and medical waste, while improving quality and creating much-needed competition. Savings to corporations alone would be as much as $174 billion annually. Today, 15 million Medicaid beneficiaries are employed. Under our plan, they and their families would receive health insurance through their employers. This would reduce the cost of the Medicaid program by 31%. We believe that our plan provides an opportunity for legislative compromise. Both liberal and moderate Democrats want a universal health care system that covers all Americans. They would like a single-payer system like Medicare-for-All or a combination of public and private payers that would cover everyone. Historically Republicans would like to reduce the federal deficit, and it is likely that they feel a more urgent need to do so with the passage of the tax cut of 2018 that is projected to increase the deficit. Efforts to reduce the federal deficit will likely in part focus on expenditures for Medicare and Medicaid. They also want to give people more choice in health care. All of these goals could be accomplished with the adoption of the Eichhorn Hutchinson Health Care Plan. Explore health insurance plans harrisburg and get the best plans for your family, if you want to know more details then please send your queries in the comment section. 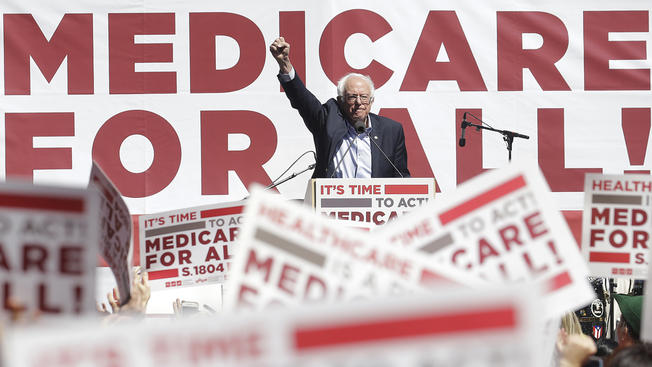 Democrats running for president will need to decide which one they're supporting or risk ending up in the muddled situation Sen. Kamala Harris, D-Calif., found herself in last weekend. Harris made a decision early in the race to run on single-payer Medicare for All, specifically a bill by Sen. Bernie Sanders, I-Vt., that would effectively replace existing private health insurance plans with a souped-up version of Medicare that covers more than the current program and requires no premiums or deductibles. Asked by CNN's Jake Tapper at a town hall in January whether she really intended to ban people's existing private coverage in favor of this new Medicare plan, Harris didn't flinch. "The idea is that everyone gets access to medical care, and you don't have to go through the process of going through an insurance company, having them give you approval, going through the paperwork, all of the delay that may require," Harris answered. "Let's eliminate all of that. Let's move on." On Sunday, speaking to Tapper again, Harris reiterated her support for the Medicare for All bill, but then turned to some more lawyer-like explanations of how she would deal with private insurance: HARRIS: I support Medicare for All, but I really do need to clear up what happened on that stage. TAPPER: Yes, OK. HARRIS: It was in the context of saying, let's get rid of all the bureaucracy. Let's get all of the waste... TAPPER: Oh, not the insurance companies? HARRIS: No. That's not what I meant. I know it was interpreted that way. If you watch the tape, I think you'll see that there are obviously many interpretations of what I said. What I meant is, let's get rid of the bureaucracy. As it relates to Medicare... TAPPER: But the bill gets rid of insurance. HARRIS: But — no, no, no, no, it does not get rid of insurance. It does not get rid of insurance. Her answer is technically accurate if you squint at it, but it's also likely to confuse voters who want to know what happens to their health care if the single-payer bill becomes law. A viewer watching might assume that Harris, by objecting to Tapper’s characterization, is saying that their own private insurance plans would not be eliminated under the Medicare for All bill she supports. That's not the case. In fact, the bill would outright ban private insurance that provides similar coverage to the new Medicare for All plans after a short transition period. That means everyone with comprehensive employee benefits or a private plan through the Affordable Care Act today would be moved onto Medicare. Get the all information about health insurance plans harrisburg pa by sending your questions in the comment section.  When a libertarian think-tank published a study of Sen. Bernie Sanders’s (I-Vt.) Medicare for All plan last month, it said that Sanders’s plan would cut payments to providers such as hospitals and doctors by 40 percent. The number suggested Sanders’s plan was wildly unrealistic, and that his plan for achieving universal health care relied on either massive cuts to doctors and hospitals or would prove far more expensive than he was otherwise saying. But Sanders’s supporters say the figure is misleading, and that doctors and hospitals could absorb cuts to their payments under the plan, which also would extend free government health insurance to every American in the country. The author of the report, the Mercatus Center’s Charles Blahous, has noted Sanders plan proposes cutting by about 40 percent the payments made by private insurers. But many providers that rely on other forms of insurance, such as Medicaid, would see their reimbursement rates go up under Sanders’s plan, or see a significantly smaller cut than the 40 percent decrease on payments from private insurers. In a recent email, Blahous said he has not calculated the overall payment cut that providers would receive from Sanders’s plan. Matt Bruenig, the founder of a socialist think-tank the People’s Policy Project, puts that number at 11 percent. The Urban Institute, a centrist think-tank, found the number is closer to 13 percent. Republicans have seized on the Mercatus study to discredit single-payer, citing its high estimates of government costs. The idea has gained increasing traction among Democratic lawmakers over the past year, winning the backing of several of its likely presidential contenders such as Sens. Kamala Harris (D-Calif.), Cory Booker (D-N.J.), and Kirsten Gillibrand (D-N.Y.). Under the current U.S. insurance system, about half the country receiving private insurance through their employer, and millions more rely on a government program such as Medicare, Obamacare, or Medicaid. Another 30 million or so Americans have no insurance. Sanders’s plan proposes moving every American in the country onto a single government-run insurer that charges no deductibles or premiums. Doing so would massively increase government expenditures -- by as much as $33 trillion by 2031, according to Blahous’s report -- while offering health insurance to the Americans who currently lack it and preventing millions more from being forced into medical bankruptcy. It would require enormous tax increases to finance, although Sanders maintains they would be offset by zeroing out every family’s spending on premiums and deductibles. In scoring Sanders’s plan, Blahous’s study produces one scenario in which it reduces national spending on health care by $2 trillion over 10 years, despite dramatic increases in government health-care expenditures. Sanders’s supporters seized on that finding, arguing it showed their plan was a bargain for the nation. But Blahous dismissed the $2 trillion in savings as unrealistic, since it would only occur under assumptions of dramatic reductions in drug prices and administrative costs, as well as the 40 percent drop in provider payments for those receiving private insurance. “Over 80 percent of hospitals would immediately be put into negative margins,” Blahous said in an email, citing data from the Centers for Medicare and Medicaid Services’s Office of the Actuary. But single-payer looks much less daunting if providers nationally face an 11 percent rather than a 40 percent cut, Sanders’s supporters say. Bruenig, of the People's Policy Project, notes one key selling point of a single-payer system is it spares physicians the reams of paperwork they have to do under the current system for private insurance companies. If America’s physicians could reduce their administrative costs to Canadian levels, he said, health care spending would fall by well over 11 percent. (Canada has a single-payer health system.) “The overhead costs here are substantially low because you don’t have to hire administrative clerks and billing experts to chase after money,” said Danielle Martin, a Toronto Women’s College Hospital physician who supports Sanders’s legislation. “What matters to people is their net income, not their reimbursement rates.” Then there are the doctors and physicians whose reimbursements would go up under single-payer. Richard Bruno, a doctor in east Baltimore who primarily sees low-income Medicaid patients, said low reimbursement rates make it difficult for his clinic to purchase the equipment he needs, like replacement microscopes. “We could do so much with higher levels of Medicaid reimbursements,” said Bruno, 38. “We’d be able to explore much better models for providing care.” But to other experts, even an 11 percent cut in provider rates could present serious challenges for private hospitals and physician practices operating on tight margins. A number of prestigious hospitals -- such as New York University, the Stanford University Medical Center, and the Ronald Reagan UCLA Medical Center -- are especially reliant on patients with private health care and would likely see average cuts bigger than 11 percent, according to Larry Levitt, a health-care expert at the Kaiser Family Foundation. “When people talk about the disruption that Medicare for All would cause, this is a big piece of it,” Levitt said. Dean Waldman, a former pediatric cardiologist at University of Chicago, doubts providers could adjust to the new reality without going out of business, noting he was able to treat many Medicaid patients in part because of the excess money brought in by patients on private plans. “When you’re talking about a 40 percent cut, you’re talking well below the cost of doing business,” said Waldman, a single-payer opponent. “The money has got to come from somewhere – and if it doesn’t, the public will simply not have doctors.” Sanders’s plan proposes slowly phasing in Medicare for All over the period of four years, giving hospitals and doctors time to adjust to the new spending levels. And his staffers do not necessarily mind the prospect of hospitals earning slightly less in the long-run, with spokesman Josh Miller-Lewis saying “this bill is not designed to make shareholders of for-profit hospitals wealthier.” But even those sympathetic to Sanders plan recognize that it may be difficult to instantly cut provider payments. Physicians across the country may not face a 40 percent pay cut, but Sanders is hoping thousands of doctors and hospitals can absorb cuts to their payment rates without going out of business. Polling from last year suggests they’re warming to the idea. “We can’t whole hog pick up a system and get it there overnight,” Linda Blumberg, a health expert at the Urban Institute, said. "Thinking of a glide path from where you are today [in provider payments] to down to something lower is going to be really critical.” You can find out more information and guidelines from health insurance companies in pa and can easily get all the details related to health insurance and medicare.  The Trump administration has ramped up its attack on the Affordable Care Act by backing a federal judge's decision to declare the entire law unconstitutional. For now, Obamacare is still standing. Around 4.1 million Americans have signed up for new plans so far this year, according to government reports, down 12% from last year. At a rally this week, Mr Trump again promised his supporters: "We are going to get rid of Obamacare." But how much has he delivered on that pledge so far? Repealing individual mandate Congressional Republicans last year finally succeeded in repealing the Obamacare requirement that people buy health insurance or pay a tax penalty. In December 2018, a federal judge in Texas ruled that the repeal of this "essential" part of the law meant the entirety of Obamacare is therefore unconstitutional. The law, however, remains in place as an appeal heads to the US Supreme Court. The mandate was not as successful as Obamacare's architects hoped in driving younger, healthier Americans into the healthcare marketplace. Now, as they ditch their coverage, analysts say insurance firms are making up for the loss by charging more to the sick or medically vulnerable patients left behind. Creating 'skinny' plans In 2018, the Trump administration allowed small businesses to offer Americans cheaper, less-comprehensive policies called Association Health Plans (AHPs) that last only up to a year. Since AHPs are short-term, companies can charge higher premiums or deny coverage based on medical history and pre-existing conditions, which Obamacare made illegal for long-term plans. These skimpy plans are meant to appeal to young, healthy Americans, but some AHPs may not cover basics like prescription drugs or maternity care. But in March 2019, a federal judge in Washington DC blocked AHPs on the grounds that they are "clearly an end-run around" to patient protections in the ACA. Shortening enrolment Initially, users had 90 days to sign up for insurance on the federal marketplace. In 2017, the Trump administration cut it down to 45 days, and then closed the website every Sunday for 12 hours, citing maintenance. Slashing ads and budgets Funding for the "navigator" programme, under which trained individuals or organisations help people sign up for insurance through Obamacare, has dropped from $62.5m (£48m) to $10m under President Trump. His administration has also cut Obamacare advertising spending to $10m - a 90% reduction. According to a November 2018 Kaiser Health poll, 61% of Americans aged 18 to 64 said they did not know about any enrolment deadlines. Ending cost-sharing reduction payments Insurance companies who covered lower-income Obamacare patients used to get cost-sharing reduction (CSR) payments from the US government. When the Trump administration cancelled these payments in October 2017, insurance firms increased premiums to compensate for the loss. The end of CSR payments had little effect on lower-income Americans, who still receive other healthcare subsidies. But it did lead to a cost hike for patients who pay full-price for their medical coverage. Medicaid work requirements The Trump administration has tried to push through work requirements for those using Medicaid - a free healthcare service for low-income Americans - saying it's a way to help end poverty. The policies are state-led and then federally approved. So far, eight states have passed rules requiring many Medicaid users to work, volunteer or train to receive benefits, US media report. On 27 March, a federal judge in Washington DC blocked "arbitrary and capricious" Trump administration-approved policies in Arkansas and Kentucky, punting them back to the Department of Health and Human Services for amending. Get insured your whole family by exploring the family health plan york and if you want to know more then please contact us in the comment section.  Life insurance can be an important part of your financial strategies, helping to ensure a more secure financial future for your loved ones when you're gone. Not only does life insurance help cover unexpected final expenses—it can also provide your family with a financial safety net or even serve as an inheritance. Some of the uses for life insurance benefits may include: Paying final costs: LifeHappens.org notes that life insurance policy benefits can be used to pay final expenses, including funeral or cremation costs, medical bills not covered by health insurance, estate administration fees or other unpaid obligations. Even expenses such as a mortgage balance can be covered by your benefit. Paying off debt or replacing income: According to LifeHappens.org, life insurance benefits can help replace your income if you pass away. Your beneficiaries can use the money to help cover essential expenses, such as paying off a mortgage or securing college educations for your children. Inheritance: The III suggests buying a policy with a named heir as a beneficiary in order to secure an inheritance for your loved ones. The death benefit can also serve as a supplement to other inheritance funds you may wish to leave your heirs. Paying federal or state estate taxes: Your heirs may face an estate tax upon receiving their inheritance, depending upon the state of residence and the amount. The III suggests that life insurance benefits may be used to partially or completely offset this cost for your heirs. Consult with your life insurance provider or a financial professional for more information on your projected estate tax impact and life insurance benefit. Charitable contributions: Life insurance policies can be created with your favorite charity as a named beneficiary, the III says. This can help ensure your philanthropic goals are met after you die, and that benefits are provided to your charity of choice — even if you don’t have a very large nest egg or estate. It is important to have a health insurance for any individual and you can check your eligibility for catastrophic health insurance pa and explore best plans for you.  Health insurance is important to have, but it's not always easy to understand. You may have to take a few steps to make sure your insurance will pay for your health care bills. There are also a lot of key words and phrases to keep straight in your head. Here's some basic info you need to know: What is insurance? Health insurance helps pay for your health care. It can help cover services ranging from routine doctor visits to major medical costs from a serious illness or injury. It also covers many preventive services to keep you healthy. You pay a monthly bill called a premium to buy your health insurance and you may have to pay a portion of the cost of your care each time you receive medical services. How do I use my policy? Each insurance company has different rules for using health care benefits. You should look at your plan’s benefits and limitations when you first sign up for insurance, especially if the plan requires you to receive your care from certain doctors and hospitals, as most plans do. In general, you will give your insurance information to your doctor or hospital when you go for care. The doctor or hospital will bill your insurance company for the services you get. WEBMD Keep Track of Your MS Symptoms Multiple sclerosis (MS) symptoms come and go. One day you're fine, but the next you may be too tired to get out of bed. Lots of things can affect the way you feel, from the weather Surgery for Parkinson's Motor Fluctuations If you can't find a way to control Parkinson's motor fluctuations -- symptoms that return after taking medicine for years -- your doctor may suggest surgery called DBS. What do I use an insurance card for? Your insurance card proves that you have health insurance. It contains information that your doctor or hospital will use to get paid by your insurance company. Doctors usually make a copy of your insurance card the first time they see you as a patient. Your card is also handy when you have questions about your health coverage. There's a phone number on it you can call for information. It might also list basics about your health plan. What's a network? Doctors and hospitals often contract with insurance companies to become part of the company's "network." The contracts spell out what they will be paid for the care they provide. If you go to a doctor in your insurance company's network, you will pay less out of your own pocket than if you go to a doctor who doesn't have a contract with your insurer. Some insurance plans will not pay anything if you do not use a network provider (except in the case of an emergency). So it is important to consult the plan’s network before seeking care. There are various health insurance companies in pa, which provides best health insurance plans for you and your family and if you want to know more then please drop your comments. |
