 What Is CHIP?
CHIP provides affordable health coverage for children of parents whose earnings are too high to qualify for Medicaid yet who cannot financially provide insurance for their children. Every state provides CHIP coverage, which sometimes includes pregnant women and parents as well. CHIP is partially funded by the federal government but is administered by the states. The benefits offered under CHIP differ from state to state, but all states’ CHIP programs provide for doctor visits, routine checkups, immunizations, prescriptions, emergency care, dental and vision care, mental health benefits, hospital care, laboratory services, and prescriptions. Qualifying and Applying for CHIP The federal government has minimum guidelines for eligibility, but states have the option to expand eligibility beyond those guidelines. CHIP is available to children under the age of 19 who are U.S. citizens, U.S. nationals, or eligible aliens. Although each state has its own rules about who qualifies for CHIP, eligibility and costs are generally based on family size and income. Parents, grandparents, or legal guardians can apply for a child’s CHIP coverage, which must be renewed annually. There are two ways to apply: by filling out an application on the Health Insurance Marketplace or by applying directly through a state’s Medicaid agency. Unlike the situation with regular individual health insurance, there is no special enrollment period, which means that parents can apply for CHIP coverage at any time of the year. CHIP and the Marketplace In some states, parents must have notably lower salaries to qualify for Medicaid for themselves than they would need to have to qualify for coverage for their children through CHIP. If children qualify for CHIP, but their parents are not eligible for Medicaid, the parents may still be able to afford coverage through the Marketplace via cost assistance savings, which are based on income. Importantly, if children are found eligible for CHIP based on their parents’ income, they will not qualify for any savings on Marketplace insurance plans. Therefore, if parents who do not qualify for Medicaid purchase a subsidized plan through the Marketplace, any of their children who are deemed eligible for Medicaid or CHIP cannot be included on the plan. Instead, their children will be part of a separate Medicaid or CHIP plan. Conclusion In contrast to the application process for individual health insurance, there is no open enrollment period for CHIP – parents can apply at any time throughout the year. CHIP coverage allows certain families to save money on their children’s health insurance while enjoying many benefits, such as mental health and hospital care. However, children who qualify for CHIP are not allowed to be included on any subsidized insurance plans that are purchased by their parents from the Marketplace.
1 Comment
 For those approaching Medicare or already covered by it, now is a critical time of year to review health benefits.
Philip Moeller — author of a popular Medicare book, “Get What’s Yours for Medicare: Maximize Your Coverage, Minimize Your Costs,” and a blogger on Medicare for the “PBS NewsHour” website — knows well about the program’s fine print that has ensnared many in what he dubs the “no one told me” syndrome. Last year, Moeller almost made a costly mistake himself. He didn’t get a chance to check his Medicare Part D drug coverage plan until one day before Medicare open season ended. He discovered that a key medication he needed had been dropped from his drug plan’s list of covered drugs. “It would have cost me $20,000 a year to buy the drug on my own,” said Moeller, who scrambled to find another plan to cover this drug and signed up just in time. Such are the complexities of Medicare that almost anyone can get snared in the fine print. Each day, about 10,000 baby boomers turn 65, making them eligible to join the 58.5 million Americans already enrolled in the national health insurance program for older Americans. Medicare now accounts for 15 percent of all federal spending, according to the Congressional Budget Office. Costs are projected to grow nearly 5 percent a year over the next decade, according to the Henry J. Kaiser Family Foundation. At this rate, Medicare Part A, which covers inpatient hospital care, short-term care in a skilled nursing facility, hospice care and some in-home care, will exceed its trust fund in 2026. For that reason, controlling Medicare costs is a big priority. In 2018, new enrollees began paying premiums based on income for Medicare Part B, which covers doctor visits, lab work, outpatient surgeries and preventive care and screenings. Several changes are coming in 2019, including to Medicare Part D drug coverage insurance and to some Medicare Advantage plans, which are offered by private insurance companies and are known as Medicare Part C. (See “Get ready for changes next year” below. ) That is why it is more important than ever for Medicare recipients — and anyone approaching age 65 — to begin looking at all the details right now, during Medicare’s open enrollment period, which began Oct. 15 and ends Dec. 7. This is the prime time of year when changes can be made in a plan without penalty. There are a lot of different plans that can work better or worse depending on your health status and finances. Experts say you should choose a plan that will not just take care of your health needs today but also what they could be in 10 years. Here are some other important elements of Medicare: 1. Most people qualify for “premium-free” Part A by having paid Medicare taxes through payroll deductions for 10 years or more. Part B premiums range from about $134 per person per month to $429 per month for those earning about $160,000 as an individual or more than $320,000 for a joint tax return. The cost of Part C Medicare Advantage plans varies by the company offering the plans and benefits covered. One other thing to know: Medicare covers most, but not all, costs. For 2018, the Part A deductible that a patient must cover is $1,340 for each hospital admission during the year. For extended hospitals stays beyond 61 days, there are additional costs of at least $335 per day that recipients pay. 2. You must sign up for Medicare when you turn 65 through the Social Security Administration, unless you are already drawing Social Security or receiving Railroad Retirement benefits, in which case enrollment may have been done for you. The clock actually starts ticking three months before your 65th birthday and ends three months after the month you were born. Enroll online or by mail, but many experts advise signing up in person at a Social Security office. Drop-ins are allowed, but it will be faster to schedule an appointment either in person or via phone by calling 800-772-1213. Delayed enrollment can result in costly penalties. How much? Up to 10 percent more per year for each year missed. You could also face a delay in the start of coverage, leaving you with a health insurance gap. One caveat: If you work at a large employer and plan to keep working, you do not have to immediately sign up for Parts B, C or D as long as you can keep an insurance plan through work. You’ll have eight months after you retire to enroll. Check with your employer and with the SSA before you turn 65. 3. Given the possibility of penalties or delayed coverage, experts say you shouldn’t wait until the last minute to sign up. A few months before retirement, ask your Human Resources department when your employer health coverage ends. Some insurance plans stop at midnight on the last day of employment, which could leave you without coverage. As you prepare to retire, ask your employer to fill out a federal form , which will verify that you have had uninterrupted, creditable health insurance coverage. 4. If you’ve been putting money in a Health Savings Account (HSA), you must stop those payments before Medicare or Social Security benefits begin. HSAs are tax-exempt accounts in which people contribute pretax dollars through their work. They are used to pay for such medical expenses as health insurance deductibles. Internal Revenue Service rules prohibit Medicare recipients from contributing to HSAs. If you continue to do so while on Medicare, you could face stiff tax penalties. But you can draw down any money left in the HSA after enrolling in Medicare or going on Social Security. Know this, however: Premium-free Part A is backdated six months from the date you apply for Medicare or Social Security. That means once it is in place, it covers costs from six months previously. So the Centers for Medicare and Medicaid Services (CMS) advises you to stop contributing to your HSA at least six months before you apply for Medicare to avoid paying tax penalties. 5. If you’ve enrolled in parts A and B, consider buying Medigap supplemental insurance. Medigap plans, which are offered by private insurers, can help cover the annual deductibles for Part A and Part B, as well as additional costs for extended hospital stays and other excess charges beyond what Medicare pays. About 14 million Americans buy a Medigap plan, according to the American Association for Medicare Supplement Insurance. Some of these plans also cover medical expenses that occur when you travel abroad. Medigap coverage can be used at any doctor or hospital accepting Medicare. 6. Medicare Advantage plans — Medicare Part C — may work better for you than signing up for the various parts of Original Medicare, so learn how they work. More than 20 million Americans annually sign up for these private insurance plans. Because they roll Parts A, B and D into one, and also can provide vision and dental coverage, some people find them easier to use and, depending on the plan chosen, less costly. If you are enrolled in a Medicare Advantage plan, you will not need a Medigap plan. Advantage plans generally require you to stay within their network of doctors and hospitals to control costs. Your choice of plans will depend on where you live; some places have 20 or more plans available, others have only one or two. 7. The cost of drugs can be a big part of health-care expenses in retirement. There are many different Part D prescription-drug coverage plans. It pays to examine the list of drugs offered by each. Find one that will match up well with your needs. Be sure to review the drug list every year during open enrollment period. If a prescription drug you need is dropped from your plan, you can switch without penalty then. You can also set up a personalized drug formulary at CMS.gov to compare Part D drug plans. Beyond the annual premium, Part D coverage requires users to pay a yearly deductible that in 2018 could not exceed $405 per person per year. Get ready for changes next year Among the changes in Medicare slated to occur in 2019 are: The Part D yearly deductible will increase by $10 to $415. The coverage gap called the “doughnut hole” will continue to shrink for brand-name prescription drugs covered by Part D insurance. (This change goes into effect for generic drugs in 2020.) The doughnut hole means that, once your drug coverage hits the yearly limit of $3,820 for 2019, you are then responsible for drug costs above that. What has changed is that you will get a 75 percent “doughnut hole discount” on brand-name drugs until your out-of-pocket costs reach the $5,100 yearly limit. Then, the Part D drug plan will resume paying for your prescription drugs. So if you hit the doughnut hole and need a brand-name medication that costs $100, you will only have to pay $25 and $95 will be applied toward your out-of-pocket spending for 2019. Starting Jan. 1, new Medicare recipients will also no longer be able to sign up for two Medigap supplemental insurance plans now offered. Medigap Plans C and F require no out-of-pocket costs for recipients. Both plans will continue operating, but since no new members will be added, current members will probably see premiums rise as the pool of people sharing costs in these plans shrinks. Some Medicare Advantage plans will begin offering coverage of lifestyle-support services, such as meals delivered at home, installation of bathroom grab bars and transportation to medical appointments. Previously, costs for such services had to be paid out of pocket. These services will be covered only if they are prescribed by a health professional. Do you have any question please contact medicare providers in pennsylvania, we will feel happy to give the answers of your questions.  We know there are many questions when it comes to figuring out your health insurance. That’s why we’ve answered some of the most important questions about the Health Insurance Marketplace below.
WHAT IS THE HEALTH INSURANCE MARKETPLACE? The Marketplace helps uninsured individuals and families find health coverage. When you fill out the Marketplace application, you will find out if you qualify for private insurance plans or Medicaid and the Children’s Health Insurance Program. Private insurance plans – We’ll tell you if you qualify for lower costs based on your household size and income. If you don’t qualify for lower costs, you can still use Marketplace to buy insurance. Plans cover essential health benefits, pre-existing conditions, and preventative care. Medicaid and the Children’s Health Insurance Program – These programs cover millions of families with limited income, disabilities, and other circumstances. If it looks like you qualify, we’ll help with the application and enrollment process. Applications for chip health insurance pa coverage can be completed at any time. WHEN IS MARKETPLACE OPEN ENROLLMENT? Marketplace Open Enrollment starts on November 1 and lasts until December 15, 2019. Enrollment must be done during this time to qualify for coverage starting January 1, 2020. If you’re interested in Medicare, another health insurance option the Family Health Clinic Navigators can help you look at, open enrollment is from October 15th through December 7th. Another health insurance option is Medicaid, and enrollment for that is open anytime. DO I HAVE TO HAVE HEALTH INSURANCE? Starting with the 2019 plan year (for which you’ll file taxes in April 2020), the Shared Responsibility Payment no longer applies. (The payment is sometimes known as the health care “mandate” or “penalty.”) If you don’t have coverage during 2019 or later, you don’t need an exemption in order to avoid the penalty. But, it’s incredibly important for you to have health insurance! No one plans to get sick or to be hurt, but you’ll like need medical care at some point. Health insurance helps to cover the costs and offers other benefits. Here are five reasons you’ll want health insurance
 If you need medical services and have insurance, now is the time to pay attention to what’s happening with your health insurance policy.
Whether you have a new insurance policy or the same insurance policy, below you will find helpful information for what to expect for your health insurance policy this year. Insurance is important because when you get medical services through in-network providers, you’ll receive these services for an agreed-upon price that’s secured through your insurance. Do you know, now you can get insurance plan for children also under the CHIP program that is Children Health Insurance Program under which they serves uninsured youths up to age 19 in families with pay too high to even think about evening consider evening think about night consider qualifying them for Medicaid. If you have a new insurance policy, what should you be aware of? On January 1st, all of your deductibles and out-of-pocket minimums are set at zero. That means you might have to pay all of the costs of your services before your plan starts paying. If you have a new insurance policy, it’s important to make sure that your current providers are in-network with your new policy. To find out if your provider is in-network, call your provider and ask if they take your specific plan. Be as specific as possible. If you have a new insurance policy and your current provider is now out-of-network, contact your insurance provider to see if they still might pay some of the cost, or you might consider finding a new provider that is in-network. Your insurance provider may not pay for the services if you receive medical services that are out-of-network. Some insurance policies now cover 100% of the cost of preventative services like a physical or a flu shot regardless of your deductible or copay. Find out what preventative services your insurance network might cover by reviewing your plan. If you have the same insurance policy, what should you expect? On January 1st, all of your deductibles and out-of-pocket minimums reset to zero. That means you might have to pay all of the costs of your services before your plan starts paying. Even if you have the same insurance policy, it is smart to review your plan because you might have access to free services that you have not taken advantage of previously. Some insurance policies now cover 100% of the cost of preventative services regardless of your deductible or copay. Every year, your insurance provider will send out new insurance cards. You can discard or shred your old card for security purposes and make sure you present your new card at pharmacies or provider offices because numbers can change. It’s important to present your newest card. If you decide you don’t like your insurance policy, what can you do? If you want to switch your insurance plan, you have to wait for the insurance open enrollment period unless you qualify for a Special Enrollment Period. Open enrollment happens only once a year (see the next section for more information on open enrollment and special enrollment.) If you know you want to switch, review your options for the next year before the open enrollment period so that when the open enrollment time comes, you have already selected a plan that you know will be best. Depending on your employer or how you get your insurance, you might have a tool to help you review how much of your plan you used in the previous year. When can you change or apply for an insurance policy?
 Medicare beneficiaries have the option to stick with Original Medicare for their healthcare services or to enroll in a Medicare Advantage plan. Advantage plans cover all of the same services as Medicare Parts A and B and can also include some extra benefits that Medicare doesn’t. Medicare Advantage plans do not cover assisted living costs, but some Advantage plans do now include benefits that are related to long-term services, such as in-home patient support, home safety modifications, and adult day care services. This came about due to some legislation passed in 2018 allowing Advantage plans to offer supplemental home services that will benefit chronically ill people. Let’s take a look at what has developed and how it’s different from what Traditional Medicare covers. Traditional Medicare and Long-Term Care OverviewOriginal Medicare covers inpatient care under Part A. This includes acute hospital care, skilled nursing care, and hospice benefits. After you’ve had a qualifying inpatient hospital stay, Part A will pay for stay in a skilled nursing facility (SNF), but only a short-term basis. This stay is capped at 100 days. After that, you pay entirely out-of-pocket. This SNF care is intended to help you recover and get back on your feet after a medical injury, illness, or procedure. So, while this care is very appropriate for someone recovering from a joint replacement or even a stroke, it is not intended to care for people who are not likely to recover. For example, if you have dementia and are not likely to return to being able to live independently, then you will transition to long-term care that you must pay for yourself. Medicare Advantage Plans and Long-Term CareMedicare Advantage plans must also cover up to 100 days in a skilled nursing facility, just like Original Medicare. However, Advantage plans have always been able to include some extras like routine dental and vision care. Going forward, they will now also be able to include supplemental home care benefits. While these are certainly not the same as full-time assisted living or nursing home care, they may help beneficiaries to remain living independently in their own homes for a longer period of time before moving into full-time assisted living.  Each Medicare Advantage insurance company can include these benefits at their own discretion. That means that some plans will offer these kinds of supplemental home care benefits and others will not.
Some of the non-medical, supplemental home health-related benefits you may begin to see some plans including are: Modifications to Improve Home Safety People often move into assisted living after they have had a fall or more difficulty getting around their own home. With this in mind, Advantage plans will now be able to offer installation of wheelchair ramps and bathroom safety grab bars. Other examples would be special air conditioners for people with breathing disorders. The hope is that if more people are able to afford these kind of home improvements, that there will be fewer medical emergencies and elderly individuals might be able to continue living at home for a longer period of time before assisted living becomes necessary. Personal Care Services in Your Own Home Generally, when people move into long-term care, it’s because they are no longer able to handle own activities of daily living like bathing, getting dressed, basic hygiene, and preparing and eating their own food. Advantage plans will be able to help by offering in-home support services for a certain amount of time each week or month. If home health aides could assist beneficiaries with some of these basic tasks as well as things like cooking and cleaning, then the Advantage plan insurance carrier may end up spending less on medical treatment. Transportation and Nutrition Support There are some Medicare beneficiaries who may no longer be able to drive and do not have access to other affordable means of transport. However, they are still able to live independently for the most part. Advantage plans will now be able to offer transportation services on a limited basis to help these individuals get to and from medical appointments and to pick up prescriptions from the pharmacy. Plans can also include delivery of hot meals to the individual at home. Each plan will be different in how often they provide these services so be sure to check the details on these services before you enroll. Adult Day Care Adult Day Care services have become tremendously popular over the last decade. This care is intended to give full-time caregivers a break or time to run other errands. The member can still receive proper care in a very safe environment. Day care centers for adults typically operate five days a week, but some may also offer services on weekends. Social interaction is a big focus for many of these facilities and the beneficiary receiving the day care may participate in crafts, exercise, games, and music therapy among other activities. Some centers may focus on medical care and/or memory care for patients as well. With the new legislation in place, we expect to see that some Advantage plans may begin to incorporate adult day care services into their plan designs. Even if an Advantage plan only offered a few days per month in adult day care, it would be a huge help to caregivers. Over the Counter Allowances While many Medicare Advantage plans include Part D medications, they do not usually include over the counter medications. Advantage plans can now begin to offer monthly or quarterly benefits that members can use to purchase vitamins, pain relievers, allergy medicines and other over the counter products. These will usually be offered in some sort of catalog that members will receive and they’ll have a set allowance to spend on these items. Telehealth Services It can sometimes be challenging for older people to make the trip to their medical provider’s office, especially if they have chronic illnesses. Advantage plans will now be able to incorporate new telehealth services that will allow members to consult their doctors via video calls on their smartphones. The Big Picture What we are seeing in these Medicare Advantage improvements is that the U.S. healthcare industry is beginning to step away from the idea of treating patients only when they are very ill. Instead they will focus on trying to prevent them from getting that ill in the first place. Insurance companies are beginning to realize that many other factors play into patient outcomes. The environment and community in which a Medicare beneficiary lives and interacts can play a critical role in how much medical spending that person’s insurance company ultimately incurs on their behalf. Will All Medicare Advantage Plans offer these benefits?There are literally thousands of Medicare Advantage plans across the country and not all of them will include all of these benefits. Instead, we can expect to see more plans beginning to include some of these benefits in 2020 and beyond. Explore blue cross medicare advantage plans and get the best options for your loved ones to choose from. if you want to know more details then please share comments in the comment section When you’ve experienced a loss and are feeling many emotions, the last thing you want to do is verify whether your insurance will cover grief counseling. Grief counseling can be just what you need to help you recover from a traumatic loss. Medicare covers several mental health services, including grief counseling. Medicare covers things like individual and group psychotherapy, family counseling, psychiatric evaluations, partial hospitalization, annual depression screenings, and medication management. However, Medicare covers each service slightly different. Be sure to read on to learn which part of Medicare covers mental health services and the costs you can expect to pay. Which part of Medicare covers grief counseling?There are two main parts of Medicare you receive your coverage from – Part A and Part B. Part A covers inpatient type services, such as inpatient stays in hospitals and skilled nursing facilities, meals while admitted, and some medications administered to you while admitted. Part B covers the bulk of your medical services. Part B covers outpatient type services, such as doctor visits, mental health services, therapy, durable medical equipment, lab work, and x-rays. Hospital status (inpatient versus outpatient) is a tricky thing to understand when it comes to Medicare. If your therapist recommends partial hospitalization as part of your treatment, you’ll live at home while commuting to the hospital for treatment. In this scenario, because you are never considered an inpatient, Part A doesn’t cover any of your treatment. Even though you’re receiving treatment at a hospital, Part B is in charge of your coverage because you’re receiving treatment on an outpatient basis. 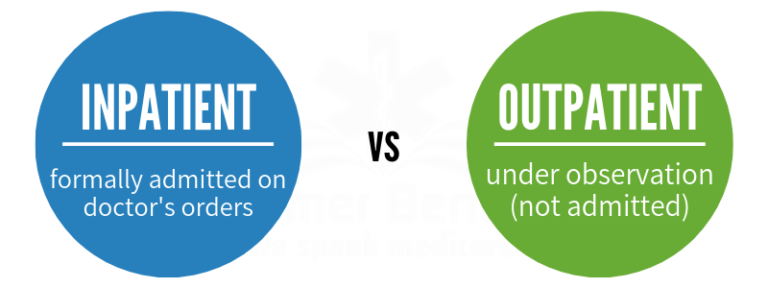 Generally, grief counseling is an outpatient service. Therefore, Part B is in charge of coverage. As long as the counseling is medically necessary, Part B will cover it for as long as you need it. Part B also covers some preventive services, such as depression screenings and wellness checks. You can receive a depression screening once every year at no charge to you. You can also get a wellness check once a year that includes an evaluation of your risk for depression. These visits are covered at 100% as long as you see a doctor who accepts Medicare assignment. Medicare’s Requirements for Grief Counseling Mental health services, including grief counseling, have a few requirements you must follow for Medicare to cover them. First, only certain types of medical professionals can administer your counseling. Medicare covers mental health services with the following type of professionals:
What is Medicare assignment?There is a maximum price that Medicare will pay for any service, also called the Medicare assignment rate. When a doctor accepts Medicare assignment, they agree to accept Medicare’s rate as the full cost for the service they provide. If a doctor accepts Medicare but doesn’t accept Medicare assignment, they can charge you, the patient, up to 15% more than Medicare’s approved rate.Other Requirements for Grief Counseling In addition to provider requirements, Medicare requires you to receive your counseling in particular settings. Part B covers grief counseling in a provider’s office, an outpatient department in a hospital, and a community mental health center. What does grief counseling cost under Medicare?The federal government regulates Medicare costs. Premiums and deductibles are adjusted each year to account for inflation and other factors. Most Americans earn premium-free Part A by working and paying Medicare taxes. However, Part B costs $135.50 per month for most beneficiaries. Like most other insurance programs, Part A and Part B have deductibles you must meet before the insurance pays anything. Part A’s deductible is per benefit period, while Part B’s deductible is per year. Part A deductible A benefit period starts the first day you are considered an inpatient. As soon as you are an inpatient, you owe the Part A deductible of $1,364 (in 2019). The benefit period ends once you have stayed out of the hospital for 60 consecutive days. For example, if you’re admitted to a hospital or mental health facility and stay for 14 days, your deductible is still in effect for the next 60 days. If you are admitted back into the hospital within those 60 days for the same reason, you won’t owe the deductible again. However, if you go 60 days without being readmitted to the hospital, you’ll owe the deductible again. Part B Deductible and Coinsurance The Part B deductible is much smaller and is only paid once per year. The Part B deductible is $185 as of 2019. Once you have your first Part B service of the year, you’ll owe $185, and Part B will cover 80% of the remaining bill. You’ll also owe the remaining 20%, which is called your coinsurance. Never pay your deductible upfront. The provider should first bill Medicare. Medicare will see you still owe your Part B deductible and will subtract that from the total bill. Part B will pay 80% of whatever is left over after the deductible. Medicare will return the bill to the provider, showing you owe the $185 deductible plus the 20% coinsurance. Let’s say your first Part B service of the year is a grief counseling session that costs $200. You owe $185 for your deductible plus $3 (your 20% coinsurance). Part B will pay the other $12. However, for your next grief counseling session, Medicare will immediately pay $160, leaving you with only $40 to pay. However, depending on the Medicare plan you have, you may not owe anything. Medicare Supplement plans and Medicare Advantage plans can lower your out-of-pocket expenses. Medicare Supplement Plans that Cover Grief Counseling Costs Medicare Supplement (Medigap) plans pay after Medicare and cover Part A and Part B costs, such as deductibles and coinsurance. There are 10 different plans to choose from. Medigap Plan B, C, D, F, and G all cover the Part A deductible and coinsurance, as well as the Part B coinsurance at 100%. So for example, if you enroll in Plan G, you would pay the Part B deductible once per year but nothing thereafter. Plan G would pick up all of the the Part B coinsurance, so you would pay nothing for your counseling. You still have to pay your Part B premium when you have a Medigap plan. Therefore, you’ll have your Part B premium and a Medigap premium. Medigap premiums can be $100/month or more depending on where you live and the cost of healthcare in that area. If a Medigap plan doesn’t fit your monthly budget, consider a Medicare Advantage plan instead.Medicare Advantage plansMedicare Advantage plans are private insurance plans that fall under Part C of Medicare. You must be enrolled in both Medicare Parts A and B to enrol in either a Medigap plan or a Medicare Advantage plan. However, because Medicare Advantage plan premiums are usually inexpensive, they’re easier to afford each month. On the other hand, you tend to have more costs on the back end with Medicare Advantage plans than you do with Medigap plans. You will owe a copay or coinsurance each time you receive a covered service. However, having a Medicare Advantage plan is usually more cost-effective than having just Original Medicare (Part A and Part B). This is because Medicare Advantage plans have out-of-pocket maximums, whereas Original Medicare does not. There is no cap to how much you can spend out-of-pocket with just Original Medicare. With a Medicare Advantage plan, you will never pay more than $6,700 (in 2019) on deductibles, copays, or coinsurance for medical services. Prepare for Grief CounselingIf you’re dealing with grief and are looking into grief counseling, follow these steps:
Most people are happy with their medicare plan. Choose the right medicare plan for yourself. If you want to know more about blue cross medicare advantage plan and the benefits of it , just drop your comments in the comment section.  The cost of health care isn’t just something impacting individuals and their families—it also affects businesses that want to prioritize employee health benefits.
Small businesses are the most vulnerable to these costs. Over the past 15 years, the per-employee cost for employers providing group health insurance increased nearly 200 percent—from around $2,200 to about $6,440. The high costs of traditional group benefits, matched only by their inconvenience and inflexibility, have prompted many small businesses to forgo offering health benefits altogether. In the current climate, this isn’t a great strategy: because unemployment rates are the lowest they’ve been in 50 years, small businesses face a competitive battle for talent in which the right health benefit is a crucial component for success. The good news is, starting in 2020, there will be more health benefit options for small businesses than ever. In this post, we’ll cover five of the most popular health benefit choices for small employers in 2020:
For each option, we’ll discuss how it works, the advantages tit offers, and what potential disadvantages a business may have to deal with if they go with one of these options. Choice 1: The qualified small employer health reimbursement arrangement (QSEHRA) The qualified small employer HRA (QSEHRA) was created in 2016 through bipartisan legislation from the federal government. With the QSEHRA, businesses with fewer than 50 employees offer their employees a monthly allowance of tax-advantaged money. The employer determines the allowance before launching the benefit. Employees choose the health care they need, like individual insurance policies, prescriptions, medical services, dental services, and more, and submit proof of their expense. The business then reimburses the employees up to their allowance amount for the cost of the services or insurance premiums. The business can include all employees or limit the benefit to only full-time employees who are automatically eligible. This allows small businesses to offer a meaningful benefit to their employees while keeping within their budget. Let’s break it down: Step 1: The small business sets a monthly allowance of tax-advantaged money to make available to each eligible employee. Step 2: Employees make purchases. They’re free to get the care, services, and/or policies that fit the needs of their families and themselves. There are a variety of expenses eligible for reimbursement. Eligible expenses include things like personal health insurance premiums, copays, deductibles, and prescription drugs. Step 3: After incurring an eligible expense, employees must submit documents to the company showing proof of the expense. The documents must show a description of the product or service, the amount billed to the employee, and the date they incurred the expense. Step 4: The business reviews and reimburses employees’ expenses. When an employee submits an expense, the business or an approved third party reviews the documentation. Then the employer reimburses the employee up to the amount of their allowance. Reimbursements provided through a QSEHRA are free of payroll taxes for businesses and their employees. Payroll taxes include social security, medicare, and unemployment tax. Reimbursements are also free of income tax for employees covered by an insurance policy that provides minimum essential coverage (MEC). The QSEHRA is often the best choice for small businesses because it’s personalized, flexible, and cost-effective. Employees can purchase what best fits their needs, while small businesses are free to keep costs within their budget. Choice 2: Individual coverage HRAs The individual coverage health reimbursement arrangement (ICHRA) was officially created by the federal government in June 2019, and is available as of January 1, 2020. Similar to a QSEHRA, an ICHRA is a company-funded, tax-free health benefit allowing businesses to reimburse their employees for personal health care expenses. Unlike other HRAs, the ICHRA is available to businesses of any size. That means small businesses as well as companies with more than 50 employees can offer an ICHRA. There are no annual allowance caps, and businesses may vary allowance amounts and eligibility by different classes of employees. Here's how it works step by step: Step 1: Through an ICHRA, businesses set a monthly allowance of tax-free money for their employees to use on individual health insurance and other health care expenses. There are no limits on annual contribution amounts, and businesses can offer different amounts to different classes of employees, including:
In general, ICHRA allowances should be the same within each class; however, distinctions can be made based on the employee’s age or family size. Step 2: Employees incur expenses for health care products and services according to their personal needs, including individual health insurance. A full list of eligible expenses can be found in IRS Publication 502. Step 3: Employees submit proof of their expenses. After incurring an expense, employees provide document to the business showing proof of the expense. The documents might be an invoice, an itemized receipt, or an explanation of benefits from their insurance provider. Step 4: The business reviews the documentation and reimburses the employees. If the documentation is sufficient and the employee’s expense is eligible to be reimbursed, the business reimburses the employee up to their allowance amount. The reimbursements are nontaxable for both the employees and the business. There are two things to keep in mind when considering an ICHRA: First, employees and their families are only eligible to participate if they have coverage under an eligible individual health insurance policy. If the employee or a participating family member fails to obtain or loses individual coverage, they cannot receive reimbursements. Second, the ICHRA comes with premium tax credit restrictions. When an employee opts to participate in the ICHRA, they’re no longer eligible to receive a premium tax credit. Employees are free to opt out and accept a tax credit instead, as long as the allowance offered was low enough that any policy would still be considered “unaffordable” and wouldn’t provide minimum value under the ACA. Choice 3: Group health insurance A group health insurance policy has traditionally been the typical choice for most businesses. Group health insurance is a plan chosen by the employer that provides coverage to employees and, in most cases, the employees’ dependents. Small businesses offering a group insurance policy to their employees pay a fixed premium to the insurance provider. They may share the cost with employees by passing on a portion of the premium. Participating employees are responsible for the copays and deductibles associated with the services they receive. Group policies also have a specific network of providers that employees can seek services from. In general, services provided by out-of-network providers are either not covered under group plans, or the percentage of the cost employees are responsible for is greater than with in-network providers. Businesses typically purchase coverage through an insurance broker or the public Small Business Health Options (SHOP) marketplaces. Traditional group health insurance can be a good choice for small businesses because employees are often already familiar with how it works and it’s relatively easy for employers to obtain. That being said, premium prices can be out of range for small businesses with a limited budget. The cost of group health insurance premiums have increased significantly in recent years and continue to climb. The least expensive policies generally have higher deductibles that put a larger burden on employees. Another downside is that employees don’t have a choice with regard to the covered network. That means they may not be able to receive services from their preferred providers. Choice 4: Self-funded health insurance In order to avoid the high cost of premiums and the restrictions associated with group health insurance, some small businesses are opting to self-insure. Through a self-insurance arrangement, businesses take on the financial responsibility for providing health care benefits to their employees. Rather than paying a fixed premium to an insurance provider, the business pays for employee’s out-of-pocket claims as they arise. The terms of eligibility and covered benefits must be outlined in formal legal plan documents. Typically, businesses set up a trust fund to earmark money and contributions are made by both the business and its employees to pay for claims. Businesses may also pair the fund with a stop-loss policy that limits the potential financial burden. Third-party administrators (TPAs) manage claims and other filings. Self-funded health insurance can help small businesses to save money, particularly in administrative costs. Savings in nonclaims expenses compared to group health insurance can range from about 10 percent to 25 percent, according to the Self-Insurance Educational Foundation. Self-insurance is risky, however. In a worst-case scenario, claims that are larger than expected could actually put a small employer out of business. For this reason, self-funded health insurance is more popular among large businesses. In fact, the average size of a business providing self-funded insurance is around 300 to 400 employees. Choice 5: Taxable stipends (informal wage increase) Due to the cost and difficulty of establishing formal legal plan documents, some small businesses choose to implement an informal wage increase, or taxable stipend. This isn’t a true health benefit, but many businesses that take this path hope it helps employees with their health care costs while avoiding complex paperwork and exorbitant premiums. With a taxable stipend, the business simply raises all employees’ wages a specific amount and tells employees the additional funds are meant for health care. There are three major downsides to this option, though: First, the funds provided to employees are taxable for both the employees and the business. Second, the business has no standing to ensure employees are utilizing the wage increase for health care. And lastly, employees aren’t likely to see the funds as an actual health benefit. Thatmay undermine the business’s intent in giving the wage increase in the first place. The future of small group health insurance Small business owners tell us every day about the challenges of trying to provide small group health insurance. Their biggest concerns are the high cost and lack of personalized options. With that in mind, it's not surprising that only 30 percent of businesses with under 50 employees offer a group insurance plan these days. This eBook provides even more details about health benefits available in 2020, including how they work, the pros and cons, and how they're implemented. We also give you a framework for deciding which benefit is the right choice for you and your small business. Going forward, we believe the choices available for small business health benefits will continue to broaden. Alternative benefits, especially HRAs, will become more accessible and small businesses will be in an even better position to provide meaningful benefits that help them succeed in the evolving market. Do you want to know more details about health insurance for small business, contact us in the comment section.  The number of health reimbursement arrangements (HRAs) currently available to employers will grow in January 2020. With all the options on the market, employers considering an HRA need to be well informed.
HRAs can be an excellent option for employers both small and large, including 501c nonprofit organizations that want to offer their W-2 employees a health benefit. In this post, we’ll discuss the most common HRA options, how they work, what the eligibility requirements are, and which option might be best for certain business goals. Let take a look at the options: 1. The QSEHRA The qualified small employer health reimbursement arrangement (QSEHRA) was created by federal legislation in December 2016. Through a QSEHRA, a small business can offer employees a monthly allowance of tax-free money to reimburse employees. The employees can be reimbursed for their insurance premiums and certain eligible out-of-pocket medical expenses like doctor visit copays, vision care, dental care, prescriptions, and more. There are limits on how much an employer is allowed to contribute through the QSEHRA in a given year. For 2019, the limit is $5,150 for single employees and $10,450 for families. Information regarding the amounts allowed to be offered in 2020 will be released by the federal government in the coming weeks. Until then, employers can expect an increase of around 3 to 5 percent from 2019 amounts. A QSEHRA is available only to qualified small employers (companies with fewer than 50 employees). The company’s full-time employees are automatically eligible to participate. The company can choose to also include part-time employees. If part-time employees are included, the benefit must be offered the same way to both employment statuses. That means all eligible employees should be offered the same allowance varying only by family status. Businesses with over 50 employees, or that offer a group plan or any other HRA, can’t offer a QSEHRA. One thing to pay attention to is how the QSEHRA coordinates with premium tax credits. If an employee that qualifies for a premium tax credit is also eligible for the QSEHRA based on their employment status, the tax credit they receive must be reduced by the amount of the QSEHRA allowance they’re offered. The QSEHRA might be best for companies:
2. The ICHRA Available starting January 2020, the individual coverage health reimbursement arrangement (ICHRA), like a QSEHRA, allows a business to offer an allowance of tax-free money for employees. Using the allowance, the business reimburses its employees up to the set allowance amount. Unlike the QSEHRA, there aren’t any annual contribution limits with the ICHRA. That means employers can offer their employees as much allowance as they want. Businesses can also limit the benefit to specific employee classes, as well as vary allowance amounts between those classes. There’s even an option to offer an allowance to the oldest employees within the same class that’s up to three times higher than the allowance offered to the youngest employees and to differ allowances within the class based on family size. The 11 ICHRA employee classes are:
One important thing to keep in mind is that businesses offering the ICHRA, can’t offer any other HRA at the same time. However, they can offer a group health insurance policy, so long as they don’t offer the same employee classes a choice between the group policy and the ICHRA. Another distinction of the ICHRA compared to other options is that for an employee to be eligible to participate, they must have individual insurance coverage. Employees can’t use a premium tax credit and participate in the ICHRA. That said, they can forgo their premium tax credit and participate, or they can opt out of the ICHRA and collect their premium tax credit if the HRA allowance amount is considered unaffordable. The ICHRA might be best suited for companies:
3. The group coverage HRA (integrated HRA) A group coverage health reimbursement arrangement (group coverage HRA), is a reimbursement plan that is available to employers of any size who offer a traditional group health insurance plan. Typically, a company offering the group coverage HRA will purchase a high-deductible group health insurance plan to save money with a lower-cost premium. The employer will then offer an annual allowance be used as a supplement to help with the amounts paid towards the group plan deductible and coinsurance. As with the ICHRA, there are no limits on annual allowances. A business offering a group coverage HRA can vary eligibility and allowances based on employee classes. The classes must be based on qualified job-based criteria (e.g., hours worked, job description, location, etc.). All employees that fall within a defined class must be treated equally with regards to allowances and eligibility. It’s important to remember that only employees who are enrolled in the group health insurance plan can participate. Employees can use the group coverage HRA to be reimbursed for out-of-pocket medical expenses like copays, prescriptions, vision care, and dental care. With group coverage HRAs, it is common for the plan to be restricted to only reimburse deductible or co-insurance expenses that are also covered under the group health insurance plan but employers can allow other qualified medical expenses to be reimbursed. To verify the employee’s expenses are eligible, an explanation of benefits (EOB) is typically required to be provided with each reimbursement request. The group HRA might be best for companies:
It’s an exciting time for businesses wanting to offer a meaningful health benefit to their employees. With so many health benefit options on the horizon for 2020, employers have the freedom to be selective. With the right information, these businesses can discern which plan will work best for their goals and be the most valuable to their employees. It is important to have group health insurance for your business and you can check your eligibility for group health insurance and explore best plans. Learning the basics of Social Security is no small feat. Your benefits will depend on many things, including how much you paid in over the years and what age you are when you apply to start your retirement benefits. Many people also get the enrollment dates and rules confused with Medicare which can further complicate your understanding of what you are eligible for.  So, here are some of the Social Security basics that all Americans should know:
Your Social Security and Medicare Eligibility Dates are Different Workers who have earned the necessary work credits can apply for Social Security retirement benefits as early as age 62. Your Medicare eligibility date, however, is later. You are eligible to sign up for both Medicare Part A and Part B at age 65, regardless of whether you have signed up for retirement income benefits yet. When you enroll in Social Security does, however, affect whether your Medicare enrollment is automatic or self-initiated.If you sign up for Social Security before age 65, Social Security will automatically enroll you into Medicare age 65. Your card will show up in your mailbox shortly before you turn 65, and your Medicare Part B premiums will be deducted from your Social Security income check each month. If you delay enrollment into Social Security, however, you will need to actively enroll in Medicare at 65. The SS office will bill you for your Part B premiums until such time that you enroll in Social Security retirement benefits. You Can Enroll in Both Social Security and Medicare at the Same WebsiteWhile you can certainly go down in person to sign up for Social Security and Medicare, many people prefer not to wait in line. You can sign up for both Medicare and your Social Security benefits online. If you are taking Social Security earlier than you become eligible for Medicare, that’s okay. You can use the website to sign up for income benefits now. Later when you turn 65, you can return to the same website to enroll in blue cross medicare advantage plan . The reverse is also true. If you are delaying enrollment into Social Security for a bigger check down the road, you can still use the SSA website to sign up for just Medicare at 65. You Need 40 Credits to Qualify for SS and Premium-Free Part ATo qualify for a Social Security Retirement benefit, you must have earned 40 credits (or quarters), which is equivalent to 10 years of earnings or work. Likewise, to qualify for premium-free Medicare Part A at age 65, you need to have the same 40 quarters of work. This needs to be employment during which FICA taxes were deducted from your paychecks to go toward your future Social Security retirement benefits and Medicare hospital benefits. People with fewer quarters may still be able to qualify for Social Security disability benefits in the event of a disability. Also, if you are married and you have the work history, but your spouse does not, your spouse can still qualify for these same two benefits under your work history. While this is the minimum you need to qualify, many retirees these days may have worked for 40 years or more. That’s okay because your benefit will be based on the highest 35 years of earnings over your work history. Enrolling in Social Security Early Will Reduce your Monthly BenefitThough you are eligible to sign up for Social Security benefits as early as age 62, there is a significant effect on your monthly income benefit level to do so. The amount of your benefit is based on your Full Retirement Age (FRA). Waiting to apply for benefits at your Full Retirement Age means you will get 100% of the benefits that you qualify for. Taking those benefits at age62 would reduce them by 25%. The reduction is permanent, so think carefully before you enroll. People born between 1943 and 1953 do not reach their FRA until they turn 66. Someone born in 1954 will reach their FRA at age 66 and 2 months. Likewise, someone born in 1955 would reach their FRA at 66 and 4 months, and so on. People born in 1960 or later will reach FRA at age 67. The main thing to keep in mind is that for every month that you take benefits before your FRA, you will be giving up a small percentage of your benefit. Delaying Enrollment into Social Security Will Increase Your Monthly BenefitJust as filing early will reduce your benefit, waiting to claim your benefits will increase them. A person whose FRA is 66 will see their Social Security check increase by 8% for each year they delay their benefits. This reaches a maximum of 32% at age 70. Waiting past age 70 will not gain you any additional benefits, so be sure to file no later than age 70. Be sure to consider that Medicare Part B premiums cost a minimum of $135.50 per person in 2019. This gets deducted monthly from your income benefits, so delaying your Social Security benefits enrollment by a year or two can significantly help to cover this cost. Delaying your enrollment into Social Security can also have an impact on your surviving spouse in the event of your death. If other eligibility requirements are met, your widow(er) can collect 100% of the benefit you were receiving or eligible to receive when he or see she reaches their Full Benefit Age. Watch out for the Earnings Limit When Filing Before your FRAMany people work well into their 60’s and even 70’s today. You can work and earn Social Security benefits at the same time, but there’s a limit. So, if you plan to work past age 62, you need to think carefully before you file early for Social Security benefits. Until you reach your FRA, earnings beyond a certain limit will cause Social Security to withhold benefits. This limit changes a bit each year, but if you think you will earn more than the limit, it may be wise to delay enrollment into Social Security benefits until you reach FRA. One piece of good news is that the benefits withheld are recalculated and added back into future benefit years. So while Social Security withholds them now, they are not forever lost. Fortunately, once you reach FRA, there are no more earnings limits. Social Security will not withhold benefits even if you earn 6 figures. Some of your Social Security earnings can be taxed though depending on how much you can earn, so be sure to consult your CPA. Your Work History Can Benefit Your SpouseEven if your spouse has never worked, he or she can still qualify for a Social Security benefit based on your work history. Your spouse will qualify for 50% of your benefit at his or her Full Retirement Age. If both spouses have worked the necessary 40 quarters, then the spousal benefits will be based on the higher-earning spouse so that you can maximize your total benefits. Keep in mind though, that spousal benefits are based on the Full Retirement Age. If your spouse decides to take his or her benefit early, that 50% benefit will be reduced. For example, let’s say Karen is eligible for a $1000 spousal benefit off Joe’s work record. Assuming her RA is 66, she needs to wait until age 66 to file for that benefit and get $1000/month. If she files early, her monthly benefit is permanently reduced. Filing at age 62 would result in a benefit of just $700/month for the long run. Ex-spouses qualify for benefits too, under certain conditions, if the marriage lasted at least 10 years. Check Your Earnings History and Estimated Benefits It’s important to check your Social Security Statement for accuracy every so often. Fortunately, that’s easier than ever to do by setting your online account at mysocialsecurity.gov. Here you will find a record of all the years of your earnings. Be sure to check for any Zero Years that may be inaccurate. Sometimes earnings information fails to post to the right place, which can result in showing that you earned nothing in a year when you know you had earnings. You can easily correct these by showing your W-2 or paystubs to Social Security. However, if you don’t know there is a Zero Year because you never check your statement, then you may no longer have W-2 records for a year that is long in the past. That’s why it’s a good idea to set up your online account and log in once a year to check it. The account also will give you an estimate of the monthly income check amount you can expect at your full retirement age, as well as the amount at age 62 and 70. You’ll want to have this information in hand whenever you meet with your financial advisor. He or she should have a good handle on these Social Security basics and can help you determine where your Social Security retirement benefits fit into the overall picture of your retirement. Medicare-for-All is sure to be the hottest topic of the upcoming Presidential elections. As an agency with tens of thousands of Medicare supplement policyholders, we get lots of questions, like “What is Medicare for All and how would it work?” There are actually a number of healthcare reform proposals that use Medicare in the name of the legislation and several presidential contenders have named their legislation specifically Medicare for All.   However, let me be clear about one thing: NONE of these proposals are anything like our current Medicare system. blue cross medicare advantage plan as it stands today – right now in 2019 – is a beloved national program that works beautifully to provide affordable coverage for tens of millions of America. It is not a single-payer system, but does have a considerable amount of federal management, rules and regulations.
The Medicare for All proposals below should really not have the word “Medicare” in them at all because it is misleading. These programs would not extend the current Medicare system to everyone. They would replace it with something very different and everyone currently on Medicare would lose the coverage they have today. Let’s look at the facts of these single-payer proposals: Medicare for All under Bernie Sanders (I-VA): S. 1129Bernie Sanders was the first to name give his proposal for healthcare reform the moniker of Medicare for All. He believes healthcare should be a human right and that the only way to ensure coverage for everyone is to offer universal coverage in the U.S. The bill establishes a national health insurance program that would be administered by the Department of Health and Human Services.x Bernie’s single-payer plan would cover all United States residents, and individuals would qualify for automatic enrollment upon birth or residency. The federal government would run the program and replace nearly all existing public and private healthcare plans. Some federal programs would continue, such as the Veterans Health Administration and Indian Health Service. This plan would cover all essential medical treatment including hospital and outpatient services, prescription drugs, mental health and substance abuse treatment, dental and vision services, and home- and community-based long-term care. This means it would cover considerably more than the current Medicare program we have in place today. Medicare, as it stands now, does not cover dental, vision, and hearing services, or long-term-care expenses. In Bernie’s ideal Medicare for All program, everyone gets free healthcare. There would be no premiums, copays, deductibles, or coinsurance for covered services except for prescription drugs. It would also ban private health insurers and allow employers to offer only coverage that is supplemental to Medicare and not duplicative of any of the benefits provided under the program. Medicare for All would free Americans from employer health coverage that may often prevent them from switching jobs. The secretary would establish the national drug formulary and would negotiate drug costs annually with the pharmaceutical manufacturers. Bernie’s proposal would allow for a 4-year transition from today’s healthcare into the new regime. It has 14 original co-sponsors. What Would Medicare for All Cost It is estimated the program would cost the United States about $3.5 trillion dollars, which would represent a 2% increase in total healthcare spending today. However, the sources of that coverage would shift from private insurance companies over to the federal government. This, of course, draws a lot of criticism as the politicians who are backing universal coverage are sometimes vague on how they propose to pay for this plan. Some of the options to fund the program that have been discussed are: A Premium Paid by Employers and Broader Self Employment TaxWe would impose a 7.5% income-based premium paid by employers. It would exempt the first $2 million in payroll to protect small businesses. Sanders’ plan would make business owners report more of their company’s income as salaries so that they would pay more self-employment taxes. A Premium Paid by All Employees Making More Than $29,000 The legislation could create a 4% income-based premium paid by employees. It would exempt the first $29,000 in income for a family of four. Eliminate Health Tax Expenditures for Businesses Since Bernie’s Medicare for All would bank employer-based health insurance, it would also get rid of employer’s deductions for the healthcare insurance they currently provide. This leaves more available dollars that can be taxed by the federal government to pay for Medicare for All. It would also eliminate Health Savings Accounts and medical expense deductions for families. A More Progressive Federal Income TaxOne proposal is to implement a marginal tax rate that goes up to 70% for those making more than $10 Million. It would also tax earned and unearned income (such as capital gains and dividends) at the same rates and limit the tax deductions available for filers who are in the very top tax bracket. If Medicare for All is passed with this funding option, the United States would have the highest income tax rate in the entire world. A More Progressive Estate TaxThis option would increase the top tax rate on inheritances, including a death tax rate of 77% for those with more than $1 billion, essentially preventing the wealthiest of families from passing on most that wealth to their heirs. A Wealth Tax In addition to the more progressive income tax, Bernie’s plan would establish an additional wealth tax on people in the top 0.1% of earnings. Collect Fees on Large Financial Institutions The law could create and collect additional fees for banks and other large financial institutions. This move is estimated to collect over $800 billion across a ten-year period. Medicare for All under Elizabeth Warren’s Medicare for All program would go one better than Bernie’s plan in that it would provide healthcare to absolutely everyone, including illegal immigrants. How Elizabeth Warren Would Pay for Medicare for All Warren claims her funding plan would not increase any middle-income class taxes, although Bernie disagrees. Her plan calls for various savings by way of reducing spending, such as redirecting taxpayer-funded health spending, stemming the growth of medical costs, reining in prescription drug costs, minimizing defense spending, and reducing insurer administrative costs. Raise Taxes on the Largest Corporations Currently, companies can deduct the cost of certain types of investments that they make into assets that \depreciate. Warren’s plan would slow the schedule of that depreciation. Tax the Top Financial Institutions Implement a fee that would apply to roughly the top 40 banks in the nation to collect an additional $100 billion over 10 years. Tax Financial Transactions Warren would also create a tax on financial transactions such as the sale of stocks and bonds to generate about $800 billion for the Medicare for All program Raise Taxes on the Top 1%Warren’s plan would include a wealth tax of 6% on people with more than $1 billion. Redirect Current Medicare/Medicaid Spending Warren claims that some of the financing for Medicare for All would come from using existing federal spending that is spent on the current Medicare and Medicaid programs.  Dive Brief:
Dive Insight: The findings build on other research showing low patient uptake of online medical records access. A paper published earlier this year by the Office of the National Coordinator for Health IT found that while more than 70% of hospitals allowed patients to view, download and transmit their health information online, two-thirds of hospitals said fewer than a quarter of patients accessed their portals. That's despite repeated attempts from CMS to highlight the issue as key to broader patient engagement and ownership of their health issues. Early this year, HHS released proposed rules to promote interoperability, curb information blocking and mandate free patient access to electronic records. The final rules are currently under review by the Office of Management and Budget and are expected to be released before the end of this year. Still, the Health Affairs study authors said the efforts haven't accomplished enough. "Overall, our findings suggest that policy efforts have failed to engage a large portion of patients in the electronic use of their data or to bridge the 'digital divide' that accompanies health care disparities," they wrote. The researchers said the results showed the effect providers can have on adoption of electronic health information and said an update to the Promoting Interoperability Program might be warranted. That program, previously called Meaningful Use, has decreased requirements for patient use and patient access over time in response to provider complaints, despite its original plan to gradually ramp up milestones. "Our study suggests that a higher threshold for both measures might be more achievable than providers claim and that CMS may wish to reconsider this decision moving forward," the researchers wrote. Get the all information about chip application pa by sending your questions in the comment section.  All women are at risk for ovarian cancer, but the greatest number of ovarian cancers occur in women 60 years or older. For women in the United States, ovarian cancer is the eighth most common cancer and the fifth leading cause of cancer death.
Ovarian cancer signs Early diagnosis is the key to survival, and the key to early diagnosis is recognizing the symptoms of ovarian cancer:
There’s no effective screening test for ovarian cancer, and it can be very hard to identify ovarian cancer early. The signs and symptoms of ovarian cancer aren’t always clear and may be hard to recognize so it’s important to pay attention to your body and know what’s normal for you. If you notice any symptoms of ovarian cancer that last for 2 weeks or longer, talk to your doctor and ask about possible causes. Something other than cancer can cause symptoms, but the only way to know is to see your health care professional. Medicare coverage for ovarian cancer screening Medicare covers many services to address your concerns, like a yearly wellness visit, bone mass measurement, cervical cancer screenings, mammograms, and cardiovascular screenings. Medicare also covers other preventive services. Talk to your doctor about risk factors, and schedule your next screening. Get expert advice and care Understanding when symptoms are a sign of something serious and either diagnosing the disease or confirming a previous diagnosis require expertise from specialists trained and experienced in treating ovarian cancer. At Medicare, our ovarian cancer experts treat all stages of the disease. If you also want to know more about blue cross medicare advantage plan just drop your comments in comment section.  Just as there are many types of people with Medicare, there are many ways for you to get information about our program. Did you know you have the right to get Medicare information in an accessible format, like Braille, large print, data/audio files, relay services and TTY communications?
While our print publications and Medicare.gov website are always available, we can also send you upon request Medicare information for free in accessible formats. Don’t worry—if you ask us for information in an accessible format and it takes a while to fulfill your request, you’ll get extra time to take action. For the best response, when you contact us, please give:
 You can buy life insurance either as an “individual” or as part of a “group” plan.
Individual Policy When you buy an individual policy, you choose the company, the plan, and the benefits and features that are right for you and your family. You might be able to buy the policy from the same agent or company representative who sells you property and liability insurance for your home, auto or business. And although you won’t qualify for any discounts by buying your life insurance and other insurance from the same representative, working with a single advisor for all your insurance needs can make your financial life simpler. Individual policies are typically sold through insurance agents or brokers. If you buy a policy through an agent or broker, you will pay a commission, also called a “load,” that is built into the premium rate. The commission compensates the agent or broker for the time spent advising you on how much and what type of life insurance to buy, for facilitating the application process, and for any further service that’s needed in future years to keep the policy up-to-date (such as changing beneficiary designations, arranging policy loans or coordinating your financial plans with your lawyer and accountant). There are two other ways to buy individual life insurance. In Connecticut, Massachusetts and New York, you can buy it from a savings bank. Or you can buy a policy directly from an insurance company or from a fee-only financial advisor—what’s known as a “no load” or “low load” policy. Although there is no sales commission on these policies, the company will still have charges built into the premium to cover its marketing expenses, application processing expenses and subsequent services. Finding an insurance company that will sell you a no-load policy isn’t easy; typing in “no load life insurance” on Internet search engines will in many cases lead you to an agent or broker. Group Policy You might have life insurance automatically from your employer; many large companies do this. Your employer also might offer you the chance to buy additional life insurance under a group policy. And you might be eligible to buy life insurance under a group policy from a union or trade association or other group you belong to (such as a college alumni association or an automobile club). Compared to buying an individual life insurance policy, there are several advantages to buying life insurance under a group policy:
Most employer group plans are term insurance, but if you leave that employer your state may require that you be allowed to convert the policy to a form of whole life insurance with the same insurance company that provides the group life insurance. You would then pay premiums directly to the company and keep the insurance in force. This can be an advantage if you are older, or have experienced deteriorating health, as it gives you the opportunity to qualify for whole life insurance without having a medical exam. Credit Life Insurance Credit cards and lending institutions may offer life insurance to pay off your outstanding loans in the event of your death. This is generally made available in two ways:
 Keeping your teeth and gums healthy is important – especially as you age. Make sure you find the best dental plan for your post-65 needs.
When I met my husband, the first thing that caught my eye was his smile. We’ve been married more than 30 years and I owe it all to those dazzling pearly whites. And you know what? He’s kept his smile looking great after all this time. Whether you’re 15, 35 or 65, it’s important to keep your mouth healthy. After all, your oral health plays a big role in your overall health. Yet, with so many factors to consider when buying a Medicare plan, it can be easy to forget about your teeth. You have two options for how you get your dental coverage. You can either find a private health plan that offers comprehensive dental coverage or buy a stand-alone dental plan. Before I get into your options, let’s get clear on what Original Medicare covers – or in this case, doesn’t. Original Medicare (the coverage you get from the government) only covers dental care that’s needed to treat an illness or injury. Basically, something really bad has to happen to your mouth for Medicare to cover it. For example, if you were in an accident and needed medically-necessary dental work, Original Medicare would likely cover it. That means the dental work you’re probably most interested in – regular checkups, fillings, cleanings and dentures – is not covered by Original Medicare. Option 1: I want to get my comprehensive dental coverage through my private health plan Depending on which private medical plan you choose (Cost, Medigap/Supplement or Medicare Advantage), you’ll find one of three things:
Comprehensive coverage may include things like regular checkups, dentures, crowns and fillings, to name a few. Be sure to check the dental benefits of the plans you compare. Option 2: I want to get my comprehensive dental coverage through a stand-alone dental plan Depending on where you live, you may be able to buy a stand-alone dental insurance plan. If this is the path you choose, be sure to:
If you’re unclear about which path may be best for you, get connected to a Medicare expert, such as a broker or Medicare insurance sales rep. They’ll be able to walk you through your options for keeping your smile bright and beautiful. If you’re retiring and your employer offers a plan from medicare providers in pennsylvania, check with your HR rep to see if your group plan includes dental coverage.  You got the card in the mail and you’re officially a Medicare member. Congrats! Are you wondering what to do next? One of your first steps is to schedule your Welcome to Medicare visit. Everyone who signs up for Medicare can get one welcome visit covered by Medicare during their first year. For the visit to be covered, make an appointment with a doctor that accepts Medicare. If you want to see the doctor you’ve been going to for years, log on to your online account and search the list of doctors your Medicare plan covers (your network) or call your insurance company to double-check that your doctor accepts your Medicare plan. What happens at a Welcome to Medicare visit?The goal of a Welcome to Medicare visit is for the doctor to get an overview of your health. You’ll talk about your current health and anything else you might want to do to stay healthy. The visit includes:
Even though your welcome visit is covered by Medicare, if your doctor recommends any extra care, tests or procedures during your visit, you might have to pay for them. You can always call your insurance company to check on the costs of these extras before you get them. What to bring The more you prepare for your visit, the easier it will be for your doctor to make health recommendations for you. Bring with you:
What’s next Once you’ve been on Medicare for more than one year, you can get one covered wellness visit each year. These visits are similar to the welcome visit and focus on keeping you healthy – both physically and emotionally – and preventing disease. Medicare and blue cross medicare advantage plan does depend on household income, meaning that, as wages rise, some families may be earning too much to qualify.  Improving the customer experience is no longer an idea that's relegated to the retail or hospitality industries. Now, the idea has gained traction across many industries, including healthcare. For health plans, improving the customer experience and providing member-centric care helps drive member acquisition and retention and improve reimbursement (via a better STARS rating).
With so many benefits at their fingertips, why haven't the majority of health plans become member-centric yet? Unfortunately, it's not that easy. Health plans need to engage both members and providers to deliver on an approach to member-centric care. However, recent developments in artificial intelligence and its applications in healthcare could provide new options for health plans looking to improve their efforts in providing member-centric care. They include: • The orchestration of the patient journey: In ZS's AI in Healthcare survey, we found that the majority of the patients (67%) feel positive about AI helping to improve the overall efficiency of healthcare. From a health plan's perspective, it means leveraging AI to better orchestrate the patient journey. This could include a data-driven way to help members pick the right coverage, find a relevant provider, make an appointment, connect to a pharmacy, etc. • Access to care: Receiving care outside of the doctor's office is gaining traction, and AI can help take it further. Our survey finds that 22% of physicians work in an organization where patients can interact with a physician virtually through a telehealth platform or an application, and 45% of the patients surveyed have received care outside of the doctor's office through devices such as computers, tablets and smartphones. Along with improving member experience, by expanding channels of care, telehealth platforms are a great way of improving utilization. • Active health management: Our survey reveals that 45% of the patients use wellness apps that track overall health and future goals. In addition, 34% of patients use wearable devices that aid or monitor daily activity to improve health and wellness. Artificial intelligence can enhance the use of wearables by providing better insights and monitoring chronic conditions in a smarter way, helping plans make their population health management initiatives more effective With AI, health plans now have a new tool to improve the customer experience, but there are a few challenges that they will have to overcome to unlock the full potential of AI in member-centric care. • Access to data: The effectiveness of an AI algorithm depends on the quality and diversity of data. Health plans need access to patient data, and the biggest challenge that patients see in AI-driven healthcare is data security, according to ZS's study. This means that plans will have to address data privacy concerns while thinking about their AI strategy. • Trust: ZS's survey also found that patients trust providers more than plans when it comes to sharing their medical and personal data. This is a tricky problem but one that plans need to solve if they want to be on the leading edge of leveraging AI in member-centric care. • Skill gap: AI expertise is isolated from the owners of the data (the payers). This might be more applicable to small- and mid-tier insurers as some of the bigger insurers have good in-house capabilities. The plans that don't have the right AI capabilities will have to put a strategy in place to overcome the expertise gap. These plans will have to decide whether to build capabilities in-house, partner or acquire companies with AI capabilities. The decision will depend on the current expertise, size of the organization, and the organization's vision about its core competencies. For get more benefits from group health, explore different plans and check your eligibility.  Dive Brief:
Dive Insight:
Get the all information about chip application pa by sending your questions in the comment section.  We have an affordability crisis in health care, and everyone should be working to bring down costs for patients. But as a new report outlines, many doctors and drugmakers have developed the coziest of relationships to keep drug costs high for their benefit.
For decades, we’ve known that pharmaceutical companies have provided gifts, meals, high-end trips, and other items of value to physicians. But drugmakers also make direct cash payments to physicians for various services provided on the drugmaker’s behalf. Now, we know the scale of the operation, and it’s breathtaking. A new investigation by ProPublica found that drugmakers and medical-device manufacturers paid doctors to the tune of more than $10 billion over five years. From 2014 to 2018, at least 700 doctors were paid more than $1 million each. Another 2,500 were paid more than $500,000 each during that time. About 600,000 physicians receive payments in any given year, and about 1 million doctors in total received payments over the last five years. (The United States has about 1.1 million physicians.) Here’s how it works. Drugmakers and medical device companies put doctors on their payroll by having them perform “consulting services,” giving a speech at a conference, or providing “educational” (i.e., promotional) talks during “lunch and learns” or “dine and dashes” at nicer local restaurants. It’s a great side gig for the doctors who can get it. What’s in it for the drug companies? The payoff comes when those doctors turn around and prescribe high-cost drugs developed by those same companies to their patients. Basically, it’s a pharma “investment” to ensure patients are prescribed the newest high-priced drugs rather than older competitors or less costly generic alternatives. And the data shows big returns for that investment. According to ProPublica, there is a direct link between these payments and the prescribing patterns of physicians. Financial arrangements, rather than patient safety or affordability, are impacting medical decisions. Many practices are employed by big pharma to keep drug costs high, but this one goes beyond simple marketing and underscores the broken incentives driving costs ever higher. Voters agree. In polls conducted by America’s Health Insurance Plans in December 2017, voters said that of all the waste and unnecessary costs in the health care system, they most want to eliminate financial incentives from drug companies that encourage doctors to prescribe a specific medicine. In 2010, building on former Supreme Court Justice Louis Brandeis’s adage that “sunlight is said to be the best of disinfectants,” federal law was changed to require these payments to be made public. But that transparency has clearly done little to change the behavior of drugmakers and doctors. When virtually everyone is engaged in the practice, what’s the incentive to stop? But when these suspect practices lead to more and pricier prescriptions of newer drugs, when other, less costly products, might work as well, it hurts patients. It also hurts taxpayers, employers, and anyone who pays health care premiums or branded drug copays. With families everywhere struggling with high drug prices, the continued costs of this practice are plainly apparent. It’s time for a clear explanation and accounting from physicians and drugmakers of the benefits. We cannot just continue along, business as usual. This is a prime example of why affordability continues to rank as the biggest problem facing Americans, and one where bipartisan solutions would appear to be achievable. It is important to have insurance for any children and you can check your eligibility for chip program and explore best plans for you.  Cervical Cancer Risk FactorsCertain risk factors can increase a woman’s chances of developing cervical cancer, including:
Cervical Cancer Screenings Save Lives According to the American Cancer Society, cervical cancer can be found early, and sometimes prevented entirely, through regular Pap and HPV tests. These screenings can also detect pre-cancers so that they are treated before they become cervical cancer. Most invasive cervical cancers are found in women who have never had a Pap test or who have not had one recently. When detected early, cervical cancer is one of the most successfully treatable cancers. In fact, thanks to the effectiveness of the Pap test, the cervical cancer death rate in the U.S. actually declined by more than 50 percent over the last 30 years. If you want to know more about blue cross medicare advantage plan just drop your comments in the comment section.  If The coverage of Preventive Care is one of the most vital parts of Medicare’s role in keeping beneficiaries healthy. Preventive Care is care that you receive to prevent illness, help detect medical conditions, and to keep you healthy. Medicare Part B covers many preventative services, such as screenings, vaccines and counseling. If you meet the eligibility requirements and guidelines for a preventative service, you must be allowed that service. This is true for both Original Medicare and Medicare Advantage Plans (MA), however coverage rules may apply.
Vaccines are a key component to helping you avoid diseases that can prevent you from aging well. Whether reinforcing the immunizations you received as a child, or preparing you for the upcoming flu season, you should have a discussion with your doctor about the four vaccines Medicare helps to pay for in order to play a proactive role with your health. ____________________________________________________________________________________________________ Influenza Vaccine
Pneumococcal Vaccine
Making the most of your Medicare Coverage: Getting vaccines is an integral part of ensuring you maintain your health as you get older, and they can also safeguard the health of your family and friends. If you know someone who may not be vaccinated, share this important information with them so they can take the steps towards protecting themselves. If you also want to know about know about Blue Cross Medicare advantage plan, just drop your comments in the comment section.  If your business is planning to offer an individual coverage health reimbursement arrangement (ICHRA), there are some important items to consider. With the creation of the ICHRA, certain regulatory guidelines were provided to ensure the plan is being administered compliantly. These guidelines range from employee eligibility to plan documents and employee notices.
This post will cover important rules businesses should keep top of mind when offering an ICHRA. 1. The ICHRA notice requirement According to federal regulation, businesses offering an ICHRA are required to adhere to a 90-day notice period before each plan year. That means, 90 days before the ICHRA’s start date, HRA administrators must notify employees about the newly available benefit and that they are eligible to participate. The 90-day notice must be provided every year the business chooses to offer the ICHRA. For employees who become newly eligible (like employees who gain eligibility after the beginning of the plan year, or newly hired employees), the notice requirement is different. A business has the option to provide the notice any time until the first day the employee’s ICHRA coverage begins. It is best practice to provide notice as soon as possible. That ensures the employee has time to review their coverage options and select an insurance plan. These are the items the notice must include:
2. ICHRA Plan documents The ICHRA is considered to be an employee health benefit, and is therefore subject to the Employee Retirement Income Security Act (ERISA). Under Section 402 of ERISA, the regulations state that every employee benefit plan must be “established and maintained pursuant to a written instrument” (ERISA, 2011). This means employee benefit plans must include a formal document defining the plan. ERISA regulation also requires that the plan document is made available to employees and their families. Along with the formal plan document, an employee health plan must also include a summary plan document (SPD). The purpose of which is to provide a summary of the full plan document to eligible employees. In general, the plan document is written in complex legal language. The SPD should be written more simply, allowing an average plan participant to reasonably understand it. While there aren’t any defined penalties for failing to meet these requirements, businesses are subject to IRS fines if participants in an ICHRA ask to see the plan document and the business doesn’t provide them one. Additionally, the business could be at risk for potential fines if an SPD is not made available to eligible employees within 120 days of the ICHRA’s creation. For employees newly enrolled in an existing ICHRA, the business has only 90 days to deliver the SPD. The ERISA requires several items to be included in the employee health plan documents. In addition to those, there are several items specific to the ICHRA that businesses should include as a best practice. Below is a list of the 10 items a business should include in their ICHRA plan documents. (Items that are legally required by ERISA are specified by an asterisk.)
3. ICHRA Eligibility Another important thing to know about the ICHRA is how employee eligibility is defined. According to ICHRA regulations, all participants must be covered by individual health insurance to participate in the benefit. In addition, a business may further structure eligibility according to 11 employee classes. They are:
A business is able to limit eligibility to employees that fall into the above-listed categories. Alternatively, a business can choose to offer the benefit to all employees without the use of classes. The spouses and dependents of eligible employees can also participate in the ICHRA, if the business allows. If the business offers a group insurance plan, it can’t be offered to the same classes of employees that are offered the ICHRA. In other words, an employee can’t be offered both the group plan and the ICHRA. The two plans must be offered exclusively. 4. Individual coverage As discussed above, eligible employees must have a qualifying individual coverage plan to participate in the ICHRA. That being said, what qualifies as individual coverage? Individual coverage is an individual health insurance policy, including on-exchange or off-exchange coverage, Medicare Parts A and B, or Medicare Part C. An employee can be the primary policyholder or they can be covered under a family member’s individual policy. Policies that aren’t considered individual coverage include the following:
5. Substantiating individual coverage Another important rule to note is that employers offering an ICHRA must take reasonable steps to ensure that eligible employees and their participating dependents are enrolled in individual health coverage. This requirement must be met at the start of each plan year, each time a reimbursement request is submitted, and on an individual basis when a newly hired employee becomes eligible. According to ICHRA regulations, individual coverage can be substantiated through one of two ways at the discretion of the plan administrator, or employer. Option 1:Employees can directly provide their employer with proof of coverage from an insurance card, explanation of benefits (EOB), or other document stating the employee (and any dependents) will have individual health coverage for the plan year or relevant month. This proof of coverage should come from a third party, like an exchange or the insurance provider. Option 2:Employees can provide a written or electronic attestation of coverage to the employer. This attestation states that the employee and their dependents will be enrolled in individual health coverage for the plan year (or relevant month). The attestation must include the date the insurance coverage begins as well as the name of the coverage provider. The final rules regarding the ICHRA state that employers or plan administrators can assume the attestation or documentation provided by the employee is valid for substantiation of individual coverage as long as the plan administrator or employer have no knowledge that it is misleading or inaccurate. Because of this, employers are not burdened with having to directly verify individual coverage for their participating employees. While the ICHRA is an amazing benefit that can help a business stay on budget, it’s important for businesses offering the plan to maintain compliance. This will ensure the business and it’s employees can enjoy the perks of the benefit without being concerned by penalties or fines. You can easily get best plans by exploring best chip application pa plans for you and your family.  The buzz around the shift of healthcare from volume to value-based care doesn’t look like it’s going to stop anytime soon. Nevertheless, people have been talking about it for a decade now, and I am just beginning to see a significant change in the space.
Right now, healthcare is more than just prescribing medicine or providing care to the patients based on their episodic requirements. It is about how every element that is associated with the field touches the lives of many and affects them for good. Moreover, some of the most affected are senior citizens. Our health underpins our happiness and is the foundation of our economic advancement; however, with the globally aging baby boomers, the challenges with the growing number of diseases need to be addressed. The modern perspective of care delivery and the rise of Medicare Advantage in the healthcare field It wouldn’t be wrong to say that the basic structure of healthcare delivery is slowly transforming with the definition of value-based care. This transition has been substantial, especially from the payer and the health plan perspective. In 2017, more than 40% of Aetna’s healthcare spending was centered on a value-based care payment model, and this number is expected to increase to 75% by 2020. On September 1, 2015, the CMS Innovation Center announced the Medicare Advantage Value-based Insurance Design (VBID) model. The initiative allowed health plans administering Medicare Advantage plans to offer targeted benefits to enrollees who have certain chronic conditions. The main goals were similar to the current major areas of focus:
The history of MA plans and the background of the Value-based Insurance Design model Since 2017, the CMS VBID Test model began testing the ability of Medicare Advantage plans to offer a better cost sharing or additional supplemental benefits to the enrollees with selected chronic conditions. CMS tested the VBID model in 7 states: Arizona, Indiana, Iowa, Massachusetts, Oregon, Pennsylvania, and Tennessee. In 2018, CMS updated the model to include Alabama, Michigan, and Texas and also allowed for VBID interventions for dementia and rheumatoid arthritis. In 2019, CMS updated the model to include organizations in 15 additional states including California, Colorado, Florida, Georgia, Hawaii, Maine, Minnesota, Montana, New Jersey, New Mexico, North Carolina, North Dakota, South Dakota, Virginia, and West Virginia, and focuses on:
A case study to depict a holistic Medicare Advantage care model Consider an example. Jane Rodriguez is a 67-year-old patient who has been suffering from Type 2 diabetes. She has Medicare Part A and Part B coverage. Additionally, she has an interesting Medicare Advantage Special Needs Plan (SNP) with built-in prescription drug coverage. Her Medicare Part B premium is $134.50, and the premium for her MA-SNP plan is $23. During one visit, Jane’s doctor advised her to increase her physical activity considering some troubles she had in the past with her drug interactions. With the additional coverage, she has been able to access a qualified care manager who created specific care plans to suit her medical and social conditions. Along with that, she has also been able to grab some impressive discounts on her medications with experts’ advice on ways to adopt a healthier lifestyle. With the coverage, she has also been able to improve her health over a period of just 2 months. Why are Medicare Advantage plans so popular among the Medicare population? Approximately one out of every three people eligible for Medicare chooses to enroll in a Medicare Advantage plan, and for good reason. MA plans have gained much attraction in recent years because of the following reasons:
Moving from ‘generic care’ to ‘focused senior care’: A step into the future of care delivery Medicare Advantage plans have long attracted senior citizens, as these plans often include benefits such as vision and dental care coverage. Such benefits are not covered in the traditional Medicare schemes. Since the Affordable Care Act of 2010, the enrollment in Medicare Advantage has increased, and 14 new companies have stepped into the domain of MA plans for 2019. The graph above indicates that the status of senior care in the United States is changing. The focus has been shifting from a ‘reactive care delivery’ to ‘preventive care delivery.’ With the growing changes in the healthcare space, it is important that every member of the patient population moves towards self-management. CMS predicts that 83% of the beneficiaries will have lower premiums in 2019 as compared to the past year. Stepping into the future of Medicare Advantage plans Based on the fact sheet released by the CMS a few days back, an exhaustive list of Medicare Advantage health plans innovation will be tested in the Value-based Insurance Design (VBID) model for the CY2020 application period. The model will be designed in such a way to:
For the CY2020 VBID application period, eligible Medicare Advantage organizations may apply to test the following interventions:
The growing trend of ‘step theory’ in the Medicare Advantage plans One of the most crucial aspects for a payer is to reduce the chances of avoidable expenditures. Step theory could be a major benefit in the cause. It is practice generally used by payers that sometimes requires the patients to try medications that are less costly instead of going for an expensive treatment. It is often called the ‘fail-first’ theory because the patients have to fail to get better with less costly drugs before stepping up for the other options. Beginning in January 2019, the private Medicare Advantage insurers have been allowed to implement step theory policies for drugs that patients receive from the providers such as infusions. This would imply that a patient’s infusion might not be the payer’s first choice to treat the disease, rather they might require to try a cheaper alternative that might have or have not worked for the patient in the past. How Medicare Advantage powers value-based initiatives Medicare Advantage plans have always been at the forefront of driving value-based care in the US healthcare space. Along with the additional Medicare advantages, it provides multiple benefits to patients. With the new initiatives by CMS, providers would need to focus on driving smarter clinical interventions to succeed in the changing landscape of the MA plans. However, the question still remains: What can providers do to deliver the best results in the field of MA plans?
Healthcare organizations should be provided with real-time insights into their patient population. With the right data at their disposal, they would be able to plan better interventions and suggest the right courses of action for their patients.
As per the new regulations, healthcare organizations can test non-uniform benefit designs to provide reduced cost-sharing or additional supplemental benefits for the Medicare Advantage enrollees based on their socioeconomic or financial condition. In this way, they would be able to target the right audience considering the non-clinical aspects instead of providing care based on clinical data alone.
Healthcare organizations can increase the patients’ access to telehealth services by allowing plans to propose the use of telehealth services instead of promoting in-person visits. Not only is this helpful in reducing the utilization cost in the network, but would also be easier for patients.
One of the required components for all the Value-based Insurance Design participating MA plans is to ensure a timely, coordinated approach to wellness and health care planning. With an efficient care management approach, providers can offer the best care services to not just the MA enrolls, but also other patients in the network. Know more about medicare providers in pennsylvania and get the best options for you and enjoy the benefits of medicare. Just drop your comments in the comment section.  Remember the adage that says you’re never too old to stop learning? Americans turning 65 should keep that in mind as their birthday approaches. For most people, reaching this milestone means becoming eligible for Medicare. And that can mean “graduating” from health insurance as you know it to a new system with its own timelines, rules, and terminology. Understanding your options and making wise choices can be daunting. Fortunately, the route to Medicare success follows a familiar path: Do your homework, don’t rush, follow directions, and seek clarification if you have a question. Below are five tips for navigating Medicare, whether you’re about to turn 65, the adult child or caregiver of someone turning 65, or a Medicare recipient interested in remedial learning. Now let’s get educated!  Know when and where to enroll You can enroll at a Social Security office or online beginning three months before turning 65 and no more than three months after to avoid late penalties that can permanently impact your premium. Those who have a disability, special condition, or receive benefits from Social Security or the Railroad Retirement Board may qualify before turning 65, or could be enrolled automatically when they’re turning 65. Determine your eligibility and calculate your premium on the official Medicare site.  Evaluate current coverage If you or your spouse are working and you’re covered by an employer’s plan, ask the benefits administrator if they require you to enroll in Medicare. If not, you can sign up later during a special enrollment period without incurring a late penalty. Also, make sure any prescription drug coverage you receive through an employer after turning 65 is creditable — deemed by Medicare to be at least equal to its drug coverage — or you’ll be on the hook for another late penalty.  Understand the Medicare basics If you’re not covered by an employer or former employer, there are two main ways to get Medicare coverage: Original Medicare (Parts A and B) – managed by the federal government. Medicare Advantage (Part C) – managed by private insurance companies to replace Original Medicare while also providing other value-added benefits. Those who choose Original Medicare must purchase separate prescription drug coverage (Medicare Part D). They can also opt for Medicare Supplement (Medigap) to work alongside Original Medicare. Original Medicare (Parts A and B) Medicare Advantage plans (Medicare Part C) are offered by health insurance companies to replace Medicare Parts A and B. Medicare Advantage covers the services provided by Original Medicare, along with dental, hearing, vision, annual physicals, and wellness benefits not covered by Original Medicare. Many Medicare Advantage plans also provide prescription drug coverage (Part D) and the convenience of having all of your Medicare benefits administered by one plan. Medicare Advantage (Part C) Most prescription drugs are not covered by Original Medicare and require a separate Medicare prescription drug plan (Medicare Part D). Some people who opt for Original Medicare also purchase Medicare Supplement (Medigap) from a private insurance company. This type of plan works alongside Original Medicare and helps pay for some uncovered medical costs, though a separate Medicare Part D plan would still be required to receive prescription drug coverage. Medicare Part A provides hospital insurance for inpatient stays, skilled nursing facilities, and hospice care. Medicare Part B provides medical insurance for doctor services, outpatient care, medical supplies, and preventive care. Parts A and B do not include many value-added benefits and services such as routine vision and dental visits, health management programs, and more. These costs would be out-of- pocket.  Avoid late penalties Failing to enroll on time can result in significant penalties, which can be permanent. Medicare Part A
Most people won’t have a premium for Part A if they paid Social Security taxes for at least 10 years while working. But those who are late and don’t meet that standard will see a 10 percent premium increase for double the length of time they were eligible but not enrolled. Example George moved to the United States from Europe and paid Social Security taxes for only a few years before turning 65. He became eligible for Part A but didn’t enroll for 18 months, so he had a 10 percent premium increase for 36 months – double the length of time he was eligible but not enrolled. Again, nearly all people turning 65 meet the standard for “premium-free Part A,” so the penalty wouldn’t apply. However, Parts B and D aren’t forgiving no matter how long you’ve paid into the system. Medicare Part B Part B carries a permanent 10-percent premium increase for each full year you are eligible but not enrolled. Example Helen was eligible for Part B for two full years before she signed up, so she has a permanent 20 percent increase (10 percent for each year) on her Part B premium. Medicare Part D The Part D penalty is also permanent and is determined by multiplying 1 percent of the “national base beneficiary premium” ($34.10 in 2016) by the number of full months you didn’t have Part D or creditable coverage. The monthly premium is rounded to the nearest $.10 and added to your monthly Part D premium. Example Tom didn’t have Part D or creditable coverage for 24 months after becoming eligible, so his 2016 penalty is 24 percent of $34.10 (the national base beneficiary premium for 2016), or $8.18. Rounded to the nearest $.10, his Part D premium increase is $8.20 per month in 2016. The total fluctuates each year with changes to the national base beneficiary premium. Remember open enrollment There is an open enrollment period, called AEP or Annual Election Period, for making changes to your Medicare Advantage or prescription drug plan that spans from Oct. 15 to Dec. 7. While you can sign up for Medicare plans up to three months before turning 65, and have the coverage begin on the first day of your birthday month, changes to your plan can only be made between those dates. AEP is not only for new enrollees. No matter how long you’ve been a Medicare recipient, open enrollment provides an opportunity to revisit your plan and make changes that reflect your current needs. Has your health changed? Are you happy with your current plan? Did you have significant out-of-pocket costs? What were these costs for? Will your current plan change in the coming year? Having these answers prior to open enrollment will help you make smart choices. If you want to know more about the medicare providers in pennsylvania then please send your queries by dropping a comment below.  Medicare’s Fall Open Enrollment is here! Officially known as the Annual Election Period (AEP) which runs from October 15 through December 7, this is main time when you can change your coverage. All changes are effective January 1 next year. If you are in a Medicare Advantage plan, you can switch plans or disenroll and return to Original Medicare. Similarly if you’re in Original Medicare and would like to join an MA plan, you can. You can also join, disenroll from or switch Medicare Part D prescription drug plans.
Each year, Medicare health plans and Part D prescription drug plans can change their premiums, deductibles, cost-sharing and some benefits, or discontinue their coverage altogether. Therefore it’s good to be aware of how your plan may change, and prepare accordingly. Some helpful preparation tips include:
To review your coverage options for 2020, you can:
|
